

Surgical strategies for older patients with glioblastoma
- PMID: 34626296
- PMCID: PMC8651607
- DOI: 10.1007/s11060-021-03862-z
Surgical strategies for older patients with glioblastoma
Erratum in
-
Correction to: Surgical strategies for older patients with glioblastoma.J Neurooncol. 2021 Dec;155(3):265. doi: 10.1007/s11060-021-03888-3. J Neurooncol. 2021. PMID: 34813021 Free PMC article. No abstract available.
Abstract
Objective: While adjuvant treatment regimens have been modified for older patients with glioblastoma (GBM), surgical strategies have not been tailored.
Methods: Clinical data of 48 consecutive patients aged 70 years or older, who underwent surgical resection for GBM with intraoperative ultrasonography (IoUS) alone or combination with intraoperative MRI (IoMRI) at Yale New Haven Hospital were retrospectively reviewed. Variables were analyzed, and comparative analyses were performed.
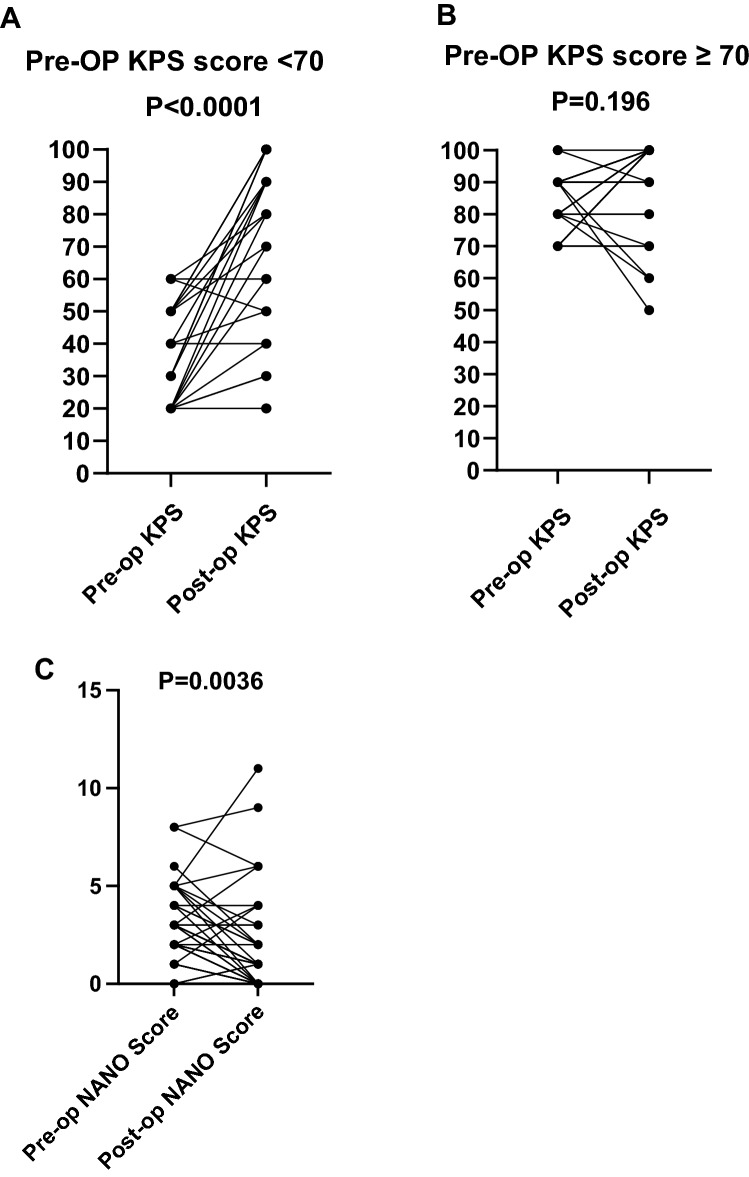
Results: The addition of IoMRI was not superior to IoUS alone in terms of overall survival (OS) (P = 0.306), Karnofsky Performance Score (KPS) at postoperative 6 weeks (P = 0.704) or extent of resection (P = 0.263). Length of surgery (LOSx), however, was significantly longer (P = 0.0002) in the IoMRI group. LOSx (P = 0.015) and hospital stay (P = 0.025) were predictors of postoperative complications. Increased EOR (GTR or NTR) (P = 0.030), postoperative adjuvant treatment (P < 0.0001) and postoperative complications (P = 0.006) were predictive for OS. Patients with relatively lower preoperative KPS scores (<70) showed significant improvement at postoperative 6 weeks (P<0.0001). Patients with complications (P = 0.038) were more likely to have lower KPS at postoperative 6 weeks.
Conclusions: Aggressive management with surgical resection should be considered in older patients with GBM, even those with relatively poor KPS. The use of ioMRI in this population does not appear to confer any measurable benefit over ioUS in experienced hands, but prolongs the length of surgery significantly, which is a preventable prognostic factor for impeding care.
Keywords: Glioblastoma; Intraoperative imaging; Neuronavigation; Surgical strategies.
© 2021. The Author(s).
Figures
References
-
- Fabbro-Peray P, Zouaoui S, Darlix A, et al. Association of patterns of care, prognostic factors, and use of radiotherapy–temozolomide therapy with survival in patients with newly diagnosed glioblastoma: a French national population-based study. J Neuro-Oncol. 2019;142(1):91–101. doi: 10.1007/s11060-018-03065-z. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
