

Pulmonary nodular lymphoid hyperplasia in a 53-year-old man with malignant sign: a case report
- PMID: 34627304
- PMCID: PMC8502387
- DOI: 10.1186/s13019-021-01672-y
Pulmonary nodular lymphoid hyperplasia in a 53-year-old man with malignant sign: a case report
Abstract
Background: Pulmonary nodular lymphoid hyperplasia (PNLH) is a rare benign illness. Due to atypical clinical and radiographic presentations, diagnosis largely depends on postoperative pathological examination. Thus, preoperative misdiagnosis is often occurred.
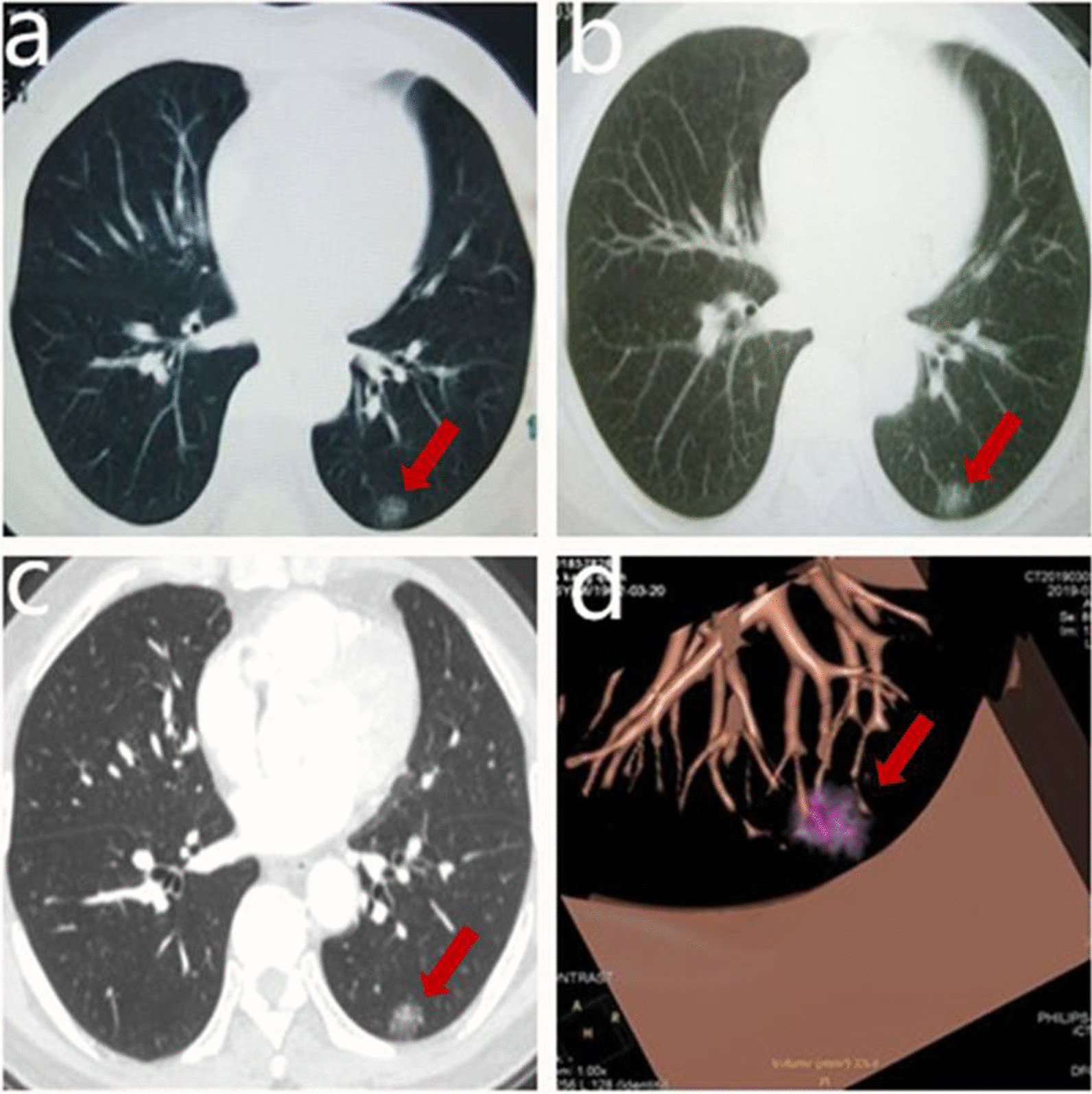
Case presentation: We present a case of asymptomatic PNLH that was seen as ground-glass opacity (GGO) on computed tomography (CT). After 3-year observation, the diagnosis tends to adenocarcinoma owing to increasing density of the node and vessel convergence sign, which were signs of malignancy. Video-assisted segmentectomy (S10) was carried out. Histopathologic examination of postoperative specimen showed follicular lymphoid hyperplasia with interfollicular lymphoplasmacytosis, consistent with PNLH. The follow-up chest CT images showed no recurrence or metastasis.
Conclusion: Although it is a benign disease, PNLH can exhibit malignant signs in the imaging examinations, which could lead to misdiagnosis. This reminds us of the uncertainty between imaging findings and diagnosis. The diagnosis depends on postoperative pathological examination. Volume doubling time is a potential parameter to differentiate PNLH from lung cancer.
Keywords: Case report; Malignant signs; Misdiagnosis; Pulmonary nodular lymphoid hyperplasia; Volume doubling time.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Bégueret H, Vergier B, Parrens M, Parrens M, Lehours P, Laurent P, Vernejoux J, Dubus P, Velly J, Mégraud F, Taytard A, Merlio J, Mascarel A. Primary lung small B-celllymphoma versus lymphoid hyperplasia: evaluation of diagnostic criteria in 26cases. Am J Surg Pathol. 2002;26(1):76–81. doi: 10.1097/00000478-200201000-00009. - DOI - PubMed
-
- Yilmaz U, Unsal I, Halilcolar H, Anar C, Yildirim Y, Sanli A, Kargi A. Nodular lymphoid hyperplasia of the lung: the role of positron emission tomography in diagnosis. Tuberk Toraks. 2009;57(4):417–421. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
