

Clinical effectiveness and safety of baricitinib for the treatment of juvenile idiopathic arthritis-associated uveitis or chronic anterior antinuclear antibody-positive uveitis: study protocol for an open-label, adalimumab active-controlled phase 3 clinical trial (JUVE-BRIGHT)
- PMID: 34627340
- PMCID: PMC8502273
- DOI: 10.1186/s13063-021-05651-5
Clinical effectiveness and safety of baricitinib for the treatment of juvenile idiopathic arthritis-associated uveitis or chronic anterior antinuclear antibody-positive uveitis: study protocol for an open-label, adalimumab active-controlled phase 3 clinical trial (JUVE-BRIGHT)
Abstract
Background: Juvenile idiopathic arthritis (JIA) is the most common pediatric rheumatic disease and the most common systemic disorder associated with uveitis in childhood. Uveitis is more common in JIA patients who are antinuclear antibody (ANA)-positive, have an early-onset disease, and have oligoarticular arthritis. JIA-associated uveitis (JIA-uveitis) is typically anterior, chronic, bilateral, nongranulomatous, and asymptomatic. Visual outcomes in JIA-uveitis have improved with current screening and treatment options; however, many patients fail to respond or do not achieve long-lasting remission. Baricitinib, an oral selective Janus kinase (JAK)1 and 2 inhibitor, may impact key cytokines implicated in the pathogenesis of JIA-uveitis or ANA-positive uveitis, representing a potential novel treatment option for disease management.
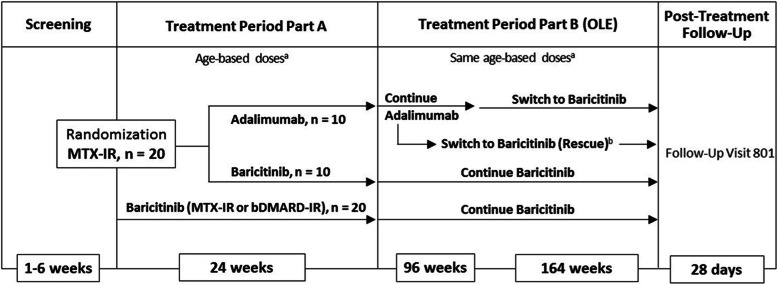
Methods: The multicenter, phase 3 trial will be conducted using an open-label Bayesian design. The study will enroll at least 20 and up to 40 patients aged 2 to <18 years with active JIA-uveitis or chronic ANA-positive uveitis without systemic features. At least 20 patients who have had an inadequate response or intolerance to methotrexate (MTX-IR), but not biologic disease-modifying antirheumatic drugs (bDMARDs), will be randomized (1:1) to open-label baricitinib or adalimumab. Approximately 20 additional patients who are MTX-IR or bDMARD inadequate responders will receive baricitinib treatment. Patients will be treated with once daily oral baricitinib at a fixed dose by age group (4 mg for patients aged ≥6 to <18 years and 2 mg for patients <6 years) or adalimumab (20 mg for patients weighing <30 kg and 40 mg for patients ≥30 kg) as a subcutaneous injection every 2 weeks. Treatment with stable background conventional synthetic DMARDs, low-dose corticosteroids, and/or nonsteroidal anti-inflammatory drugs is allowed. The primary endpoint is the proportion of patients with response at week 24. Patients may continue treatment for up to 5 years.
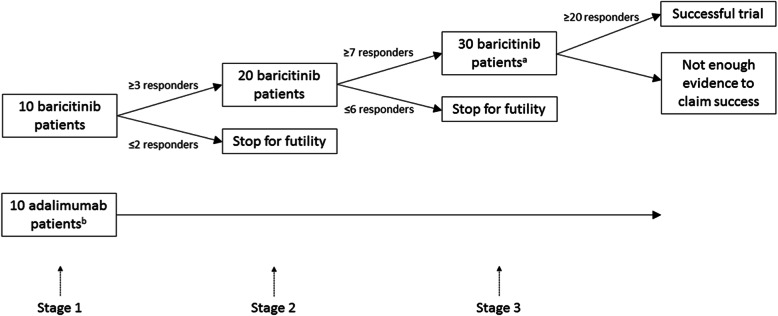
Discussion: This is the first pediatric clinical trial to assess the clinical effectiveness and safety of a JAK inhibitor in JIA-uveitis or chronic ANA-positive uveitis. A novel Bayesian design is used to assess the efficacy of baricitinib, including an adalimumab reference arm, in this small patient population with unmet medical need.
Trial registration: EudraCT 2019-000119-10 . Registered on January 4, 2019; NCT04088409 . Registered on September 12, 2019.
Keywords: Antinuclear antibody-positive; Baricitinib; Bayesian analysis; Juvenile idiopathic arthritis; Open-label Bayesian design; Ophthalmology; Pediatric; Randomized controlled trials; Rheumatology; Uveitis.
© 2021. The Author(s).
Conflict of interest statement
AVR has received consultancies and/or speaking fees from AbbVie, Roche, UCB, Eli Lilly and Company, and Sobi. CMG has received consultancies and/or speaking fees from Eli Lilly and Company and Novartis. SYK, DES, SdB, and RL are employees and may be shareholders of Eli Lilly and Company. PQ has received consultancies and/or speaking fees from AbbVie, BMS, Chugai-Roche, Eli Lilly and Company, Novartis, Novimmune, and Sobi and served on two data safety monitoring boards for Sanofi.
Figures
References
-
- Ravelli A, Felici E, Magni-Manzoni S, Pistorio A, Novarini C, Bozzola E, Viola S, Martini A. Patients with antinuclear antibody-positive juvenile idiopathic arthritis constitute a homogeneous subgroup irrespective of the course of joint disease. Arthritis Rheum. 2005;52(3):826–832. doi: 10.1002/art.20945. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
