

Physical, cognitive, and mental health impacts of COVID-19 after hospitalisation (PHOSP-COVID): a UK multicentre, prospective cohort study
- PMID: 34627560
- PMCID: PMC8497028
- DOI: 10.1016/S2213-2600(21)00383-0
Physical, cognitive, and mental health impacts of COVID-19 after hospitalisation (PHOSP-COVID): a UK multicentre, prospective cohort study
Erratum in
-
Correction to Lancet Respir Med 2021; 9: 1275-87.Lancet Respir Med. 2022 Jan;10(1):e9. doi: 10.1016/S2213-2600(21)00540-3. Epub 2021 Dec 1. Lancet Respir Med. 2022. PMID: 34863334 Free PMC article. No abstract available.
-
Correction to Lancet Respir Med 2021; 9: 1275-87.Lancet Respir Med. 2024 Jun;12(6):e41. doi: 10.1016/S2213-2600(24)00142-5. Lancet Respir Med. 2024. PMID: 38821685 Free PMC article. No abstract available.
Abstract
Background: The impact of COVID-19 on physical and mental health and employment after hospitalisation with acute disease is not well understood. The aim of this study was to determine the effects of COVID-19-related hospitalisation on health and employment, to identify factors associated with recovery, and to describe recovery phenotypes.
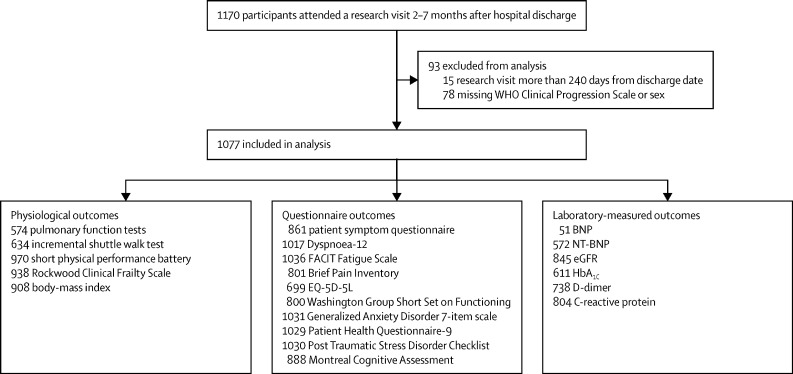
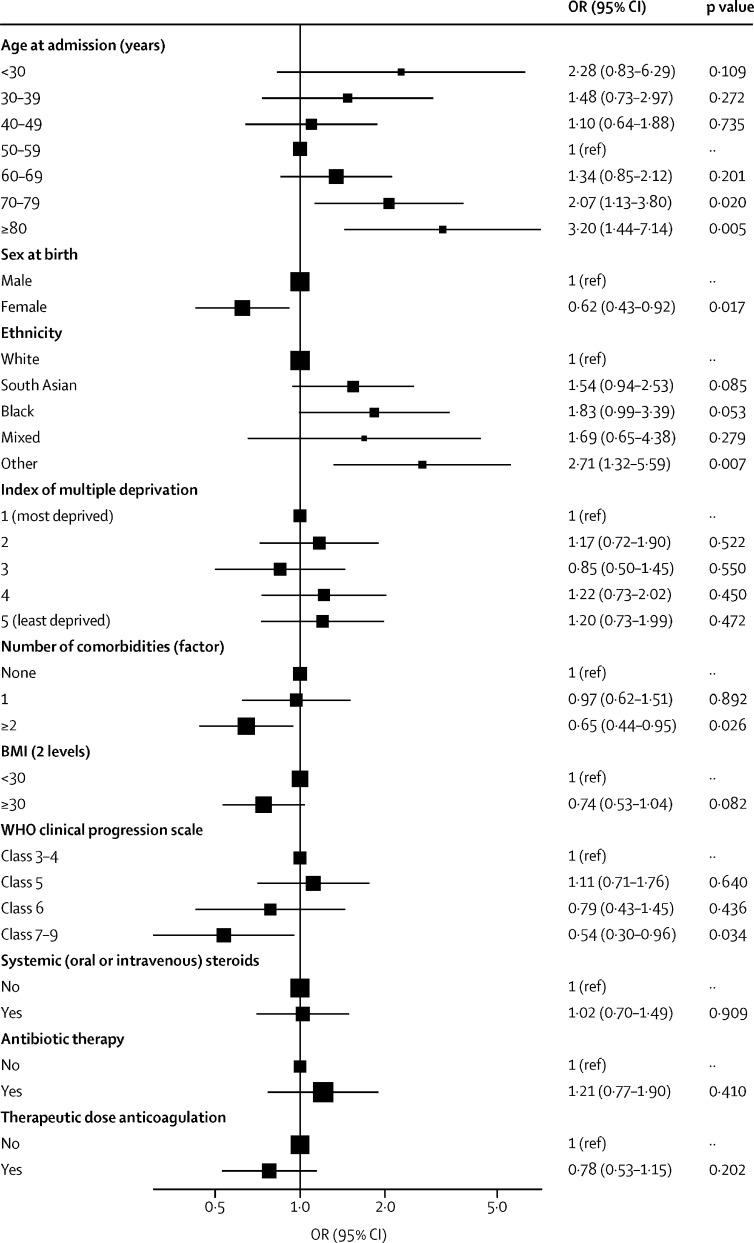
Methods: The Post-hospitalisation COVID-19 study (PHOSP-COVID) is a multicentre, long-term follow-up study of adults (aged ≥18 years) discharged from hospital in the UK with a clinical diagnosis of COVID-19, involving an assessment between 2 and 7 months after discharge, including detailed recording of symptoms, and physiological and biochemical testing. Multivariable logistic regression was done for the primary outcome of patient-perceived recovery, with age, sex, ethnicity, body-mass index, comorbidities, and severity of acute illness as covariates. A post-hoc cluster analysis of outcomes for breathlessness, fatigue, mental health, cognitive impairment, and physical performance was done using the clustering large applications k-medoids approach. The study is registered on the ISRCTN Registry (ISRCTN10980107).
Findings: We report findings for 1077 patients discharged from hospital between March 5 and Nov 30, 2020, who underwent assessment at a median of 5·9 months (IQR 4·9-6·5) after discharge. Participants had a mean age of 58 years (SD 13); 384 (36%) were female, 710 (69%) were of white ethnicity, 288 (27%) had received mechanical ventilation, and 540 (50%) had at least two comorbidities. At follow-up, only 239 (29%) of 830 participants felt fully recovered, 158 (20%) of 806 had a new disability (assessed by the Washington Group Short Set on Functioning), and 124 (19%) of 641 experienced a health-related change in occupation. Factors associated with not recovering were female sex, middle age (40-59 years), two or more comorbidities, and more severe acute illness. The magnitude of the persistent health burden was substantial but only weakly associated with the severity of acute illness. Four clusters were identified with different severities of mental and physical health impairment (n=767): very severe (131 patients, 17%), severe (159, 21%), moderate along with cognitive impairment (127, 17%), and mild (350, 46%). Of the outcomes used in the cluster analysis, all were closely related except for cognitive impairment. Three (3%) of 113 patients in the very severe cluster, nine (7%) of 129 in the severe cluster, 36 (36%) of 99 in the moderate cluster, and 114 (43%) of 267 in the mild cluster reported feeling fully recovered. Persistently elevated serum C-reactive protein was positively associated with cluster severity.
Interpretation: We identified factors related to not recovering after hospital admission with COVID-19 at 6 months after discharge (eg, female sex, middle age, two or more comorbidities, and more acute severe illness), and four different recovery phenotypes. The severity of physical and mental health impairments were closely related, whereas cognitive health impairments were independent. In clinical care, a proactive approach is needed across the acute severity spectrum, with interdisciplinary working, wide access to COVID-19 holistic clinical services, and the potential to stratify care.
Funding: UK Research and Innovation and National Institute for Health Research.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests JDC reports grants and personal fees from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Novartis, and Insmed, personal fees from Chiesi, Zambon, Janssen, and Grifols, and grants from Gilead Sciences, outside the submitted work. TC reports grants from Guy's and St Thomas' Charity, fees from workshops, and fees from writing self-help books on fatigue, outside the submitted work. NE received a donation of SARS-CoV-2 lateral flow antigen test kits from Mologic, in relation to an unrelated COVID-19 project. Neither NE nor his institution have received any financial compensation and he has no financial relationship of any kind with Mologic. RAE reports grants from GlaxoSmithKline during the conduct of the study; and grants from the National Institute for Health Research (NIHR) and personal fees from GlaxoSmithKline, AstraZeneca, and Chiesi, outside the submitted work. AH reports personal fees from Vertex Pharmaceuticals, Mylan Healthcare, and the Cystic Fibrosis Foundation, and grants from JP Moulton Trust and NIHR, outside the submitted work. LGH reports receiving sponsorship for attending international scientific meetings from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, and Napp Pharmaceuticals, personal fees from Novartis, Hoffman la Roche/Genentech, Sanofi, Evelo Biosciences, GlaxoSmithKline, AstraZeneca, Teva, Theravance, and Circassia, and grants from Medimmune, Novartis UK, Roche/Genentech, GlaxoSmithKline, Amgen, Genentech/Hoffman la Roche, AstraZeneca, Medimmune, Aerocrine, and Vitalograph, outside the submitted work. NH reports that his research group has received unrestricted grants (managed by Guy's & St Thomas' Foundation Trust) from Philips and Resmed. Philips are contributing to the development of the MYOTRACE technology. SH reports personal fees and fees to institution for advisory boards and consultancy from Novo Nordisk, Eli Lilly, Zealand Pharma, and Sanofi Aventis, outside the submitted work. JJ reports personal fees from Boehringer Ingelheim, Roche, GlaxoSmithKline, and NHSX, outside the submitted work. RGJ reports personal fees and research funding from Biogen, personal fees from Galapagos, Heptares, Boehringer Ingelheim, Pliant, Roche/InterMune, MedImmune, PharmAkea, Bristol Myers Squibb, Chiesi, Roche/Promedior, Veracyte, and GlaxoSmithKline research funding from Galecto, collaborative award from RedX and Nordic Biosciences, and was an advisory board member for NuMedii, outside the submitted work. RGJ is supported by an NIHR Professorship (RP-2017-08-ST2-014) and is a trustee for Action for Pulmonary Fibrosis. GM reports grants from AstraZeneca, outside the submitted work. PJMO reports grants from the Medical Research Council (MRC), the EU, and NIHR, and personal fees from Pfizer, Nestle, and Janssen, outside the submitted work. PP reports a grant from NIHR, outside the submitted work. MRo reports a senior clinical fellowship as part of research training and a 1-year post working in Pharma Development Neurosciences with Roche Pharmaceuticals, outside the submitted work. ADS reports grants and personal fees from AstraZeneca, Bayer, Boehringer, Chiesi, Forest Laboratories, GlaxoSmithKline, Grifols, Insmed, MedImmune, Novartis, Pfizer, and 30T, outside the submitted work. MGS reports grants from NIHR, MRC, and the Health Protection Research Unit in Emerging & Zoonotic Infections, University of Liverpool, during the conduct of the study; and reports being a minority owner and chair of the infectious disease scientific advisory board for Integrum Scientific, outside the submitted work. AShe reports being a Member of the Scottish Government's Chief Medical Officer's COVID-19 Advisory Group. MT reports personal fees from Merck Sharp & Dohme and GlaxoSmithKline, and grants and personal fees from Bayer and Actelion, during the conduct of the study. LVW reports grants from GlaxoSmithKline and Orion, outside the submitted work. All other authors declare no competing interests.
Figures

Comment in
-
Surviving COVID-19: a familiar road to recovery?Lancet Respir Med. 2021 Nov;9(11):1211-1213. doi: 10.1016/S2213-2600(21)00447-1. Epub 2021 Oct 7. Lancet Respir Med. 2021. PMID: 34627561 Free PMC article. No abstract available.
References
-
- Public Health England Coronavirus (COVID-19) in the UK. https://coronavirus.data.gov.uk
-
- Desai SV, Law TJ, Needham DM. Long-term complications of critical care. Crit Care Med. 2011;39:371–379. - PubMed
-
- Office for National Statistics National statistics postcode lookup (February 2020) February, 2020. https://geoportal.statistics.gov.uk/datasets/national-statistics-postcod...
Publication types
MeSH terms
Grants and funding
- MC_UU_12014/8/MRC_/Medical Research Council/United Kingdom
- 209553/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- MR/V027859/1/MRC_/Medical Research Council/United Kingdom
- MR/T005580/1/MRC_/Medical Research Council/United Kingdom
- MC_PC_19026/MRC_/Medical Research Council/United Kingdom
- MC_PC_19059/MRC_/Medical Research Council/United Kingdom
- G1000191/MRC_/Medical Research Council/United Kingdom
- MC_UU_00008/11/MRC_/Medical Research Council/United Kingdom
- MR/S019669/1/MRC_/Medical Research Council/United Kingdom
- MC_PC_20016/MRC_/Medical Research Council/United Kingdom
- 206330/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- CH/1999001/11735/BHF_/British Heart Foundation/United Kingdom
- SP/17/16/33519/BHF_/British Heart Foundation/United Kingdom
- MR/P021220/1/MRC_/Medical Research Council/United Kingdom
- FS/18/13/33281/BHF_/British Heart Foundation/United Kingdom
- MC_PC_19025/MRC_/Medical Research Council/United Kingdom
- MR/L018942/1/MRC_/Medical Research Council/United Kingdom
- G0600520/MRC_/Medical Research Council/United Kingdom
- G0700859/MRC_/Medical Research Council/United Kingdom
- SP/14/6/31350/BHF_/British Heart Foundation/United Kingdom
- G0501425/MRC_/Medical Research Council/United Kingdom
- G0801952/MRC_/Medical Research Council/United Kingdom
- MR/M008894/1/MRC_/Medical Research Council/United Kingdom
- CH/16/1/32013/BHF_/British Heart Foundation/United Kingdom
- G1001046/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
