

AGO Recommendations for the Surgical Therapy of the Axilla After Neoadjuvant Chemotherapy: 2021 Update
- PMID: 34629490
- PMCID: PMC8494519
- DOI: 10.1055/a-1499-8431
AGO Recommendations for the Surgical Therapy of the Axilla After Neoadjuvant Chemotherapy: 2021 Update
Erratum in
-
Correction: AGO Recommendations for the Surgical Therapy of the Axilla After Neoadjuvant Chemotherapy: 2021 Update.Geburtshilfe Frauenheilkd. 2021 Oct 22;81(10):e31. doi: 10.1055/a-1674-1114. eCollection 2021 Oct. Geburtshilfe Frauenheilkd. 2021. PMID: 34720743 Free PMC article.
Abstract
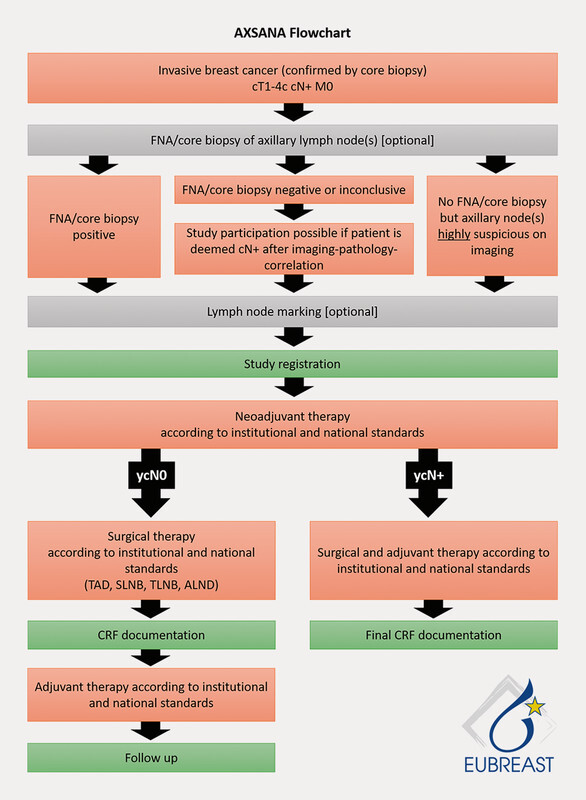
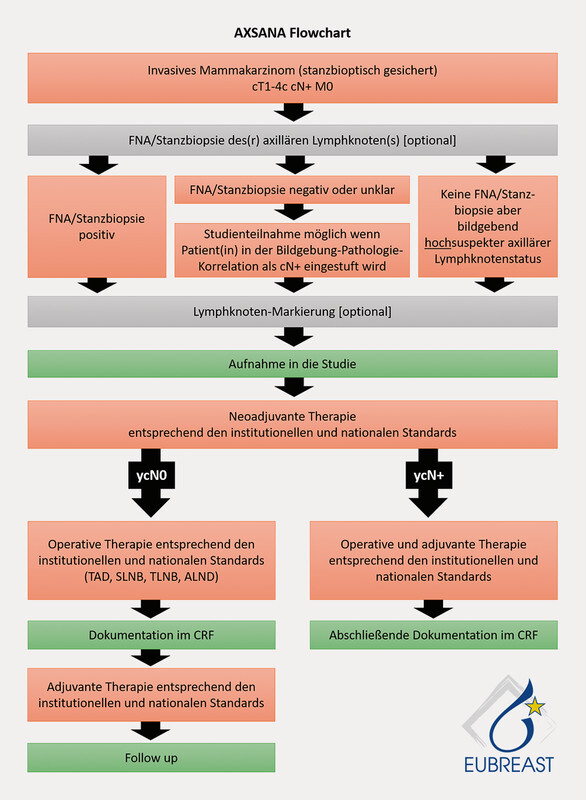
For many decades, the standard procedure to treat breast cancer included complete dissection of the axillary lymph nodes. The aim was to determine histological node status, which was then used as the basis for adjuvant therapy, and to ensure locoregional tumour control. In addition to the debate on how to optimise the therapeutic strategies of systemic treatment and radiotherapy, the current discussion focuses on improving surgical procedures to treat breast cancer. As neoadjuvant chemotherapy is becoming increasingly important, the surgical procedures used to treat breast cancer, whether they are breast surgery or axillary dissection, are changing. Based on the currently available data, carrying out SLNE prior to neoadjuvant chemotherapy is not recommended. In contrast, surgical axillary management after neoadjuvant chemotherapy is considered the procedure of choice for axillary staging and can range from SLNE to TAD and ALND. To reduce the rate of false negatives during surgical staging of the axilla in pN+ CNB stage before NACT and ycN0 after NACT, targeted axillary dissection (TAD), the removal of > 2 SLNs (SLNE, no untargeted axillary sampling), immunohistochemistry to detect isolated tumour cells and micro-metastases, and marking positive lymph nodes before NACT should be the standard approach. This most recent update on surgical axillary management describes the significance of isolated tumour cells and micro-metastasis after neoadjuvant chemotherapy and the clinical consequences of low volume residual disease diagnosed using SLNE and TAD and provides an overview of this year's AGO recommendations for surgical management of the axilla during primary surgery and in relation to neoadjuvant chemotherapy.
Keywords: breast cancer; neoadjuvant chemotherapy; sentinel LNE; targeted axillary dissection.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest/Interessenkonflikt PD DR Banys-Paluchowski: Honoraria for lectures and advisory role from Lilly, Pfizer, Roche, Amgen, Eisai, Astra Zeneca, Daiichi Sankyo, Novartis, GSK and study support from Endomag, Merit Medical and Mammotome. Prof. Dr. V. Müller: VM received speaker honoraria from Amgen, Astra Zeneca, Daiichi Sankyo, Eisai, GSK, Pfizer, MSD, Novartis, Roche, Teva, Seagen and consultancy honoraria from Genomic Health, Hexal, Roche, Pierre Fabre, Amgen, ClinSol, Novartis, MSD, Daiichi Sankyo, Eisai, Lilly, Seagen. Institutional research support from Novartis, Roche, Seagen, Genentech. Travel grants: Roche, Pfizer, Daiichi Sankyo./ Vortragshonorare: Amgen, Astra Zeneca, Daiichi Sankyo, Eisai, Pfizer, MSD, Novartis, Roche, Teva, Seattle Genetics, GSK, Seagen. Beratertätigkeit: Genomic Health, Hexal, Roche, Pierre Fabre, Amgen, ClinSol, Novartis, MSD, Daiichi Sankyo, Eisai, Lilly, GSK, Tesaro, Seagen und Nektar. Forschungsuntersützung an den Arbeitgeber: Novartis, Roche, Seattle Genetics, Genentech. Reisekosten: Roche, Pfizer, Daiichi Sankyo.
Figures


References
-
- Kühn T, Klauss W, Darsow M. Long-term morbidity following axillary dissection in breast cancer patients – clinical assessment, significance for life quality and the impact of demographic, oncologic and therapeutic factors. Breast Cancer Res Treat. 2000;64:275–286. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials