

Screening for nonalcoholic fatty liver disease-when, who and how?
- PMID: 34629804
- PMCID: PMC8475001
- DOI: 10.3748/wjg.v27.i35.5803
Screening for nonalcoholic fatty liver disease-when, who and how?
Abstract
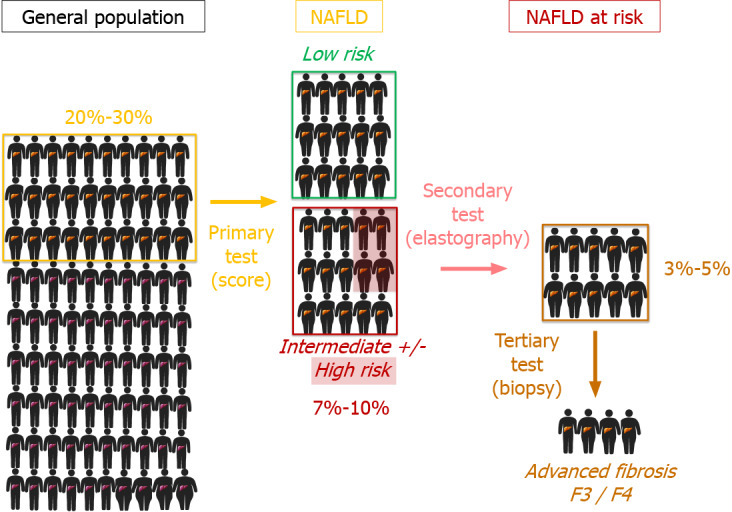
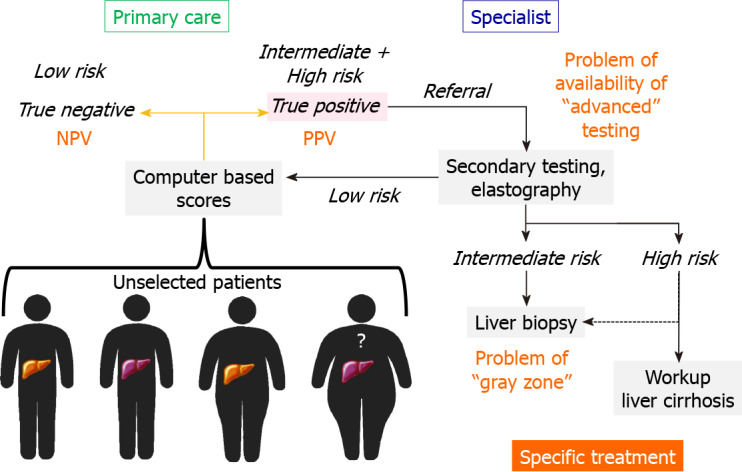
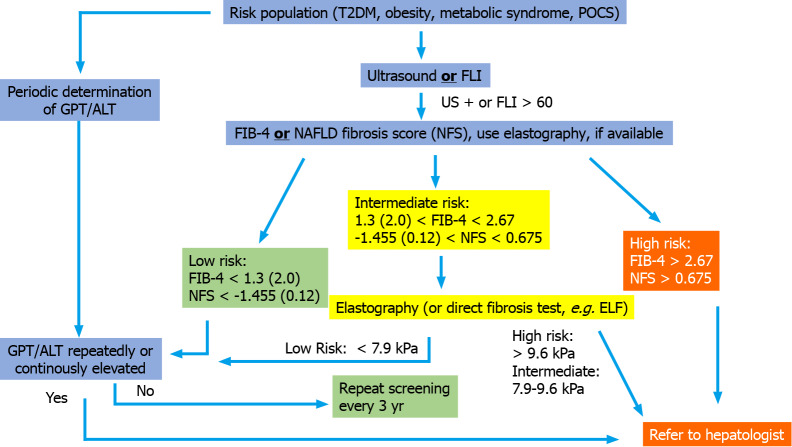
Nonalcoholic fatty liver disease (NAFLD) is becoming a frequent liver disease, especially in patients with metabolic syndrome and especially in Western countries. Complications of NAFLD comprise progressive fibrosis, cirrhosis and hepatocellular carcinoma. NAFLD also represents an independent risk factor for cardiovascular disease, extrahepatic neoplasia and other organ damage, such as renal insufficiency. Given the epidemiological importance of the disease, new developments in specific treatment of the disease and the wide availability of noninvasive techniques in estimating steatosis and fibrosis, NAFLD should be subject to screening programs, at least in countries with a high prevalence of the disease. The review discusses prerequisites for screening, cost-effectiveness, current guideline recommendations, suitability of techniques for screening and propositions for the following questions: Who should be screened? Who should perform screening? How should screening be performed? It is time for a screening program in patients at risk for NAFLD.
Keywords: Cirrhosis; Diabetes; Liver fibrosis; Nonalcoholic fatty liver disease; Screening.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: CGD reports personal speaker fees from Falk Foundation. MR declares no conflict of interest. AG serves as advisor and steering committee member for AbbVie, Alexion, Bayer, BMS, CSL Behring, Eisai, Gilead, Intercept, Ipsen, Merz, MSD, Novartis, Pfizer, Roche, Sanofi-Aventis, Sequana and as speaker for AbbVie, Alexion, BMS, CSL Behring, Falk, Gilead, Intercept, Merz, MSD, Novartis, Roche, Sequana. AG also received research support from Intercept and Falk (NAFLD CSG), Novartis.
Figures
References
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84. - PubMed
-
- Eslam M, Newsome PN, Sarin SK, Anstee QM, Targher G, Romero-Gomez M, Zelber-Sagi S, Wai-Sun Wong V, Dufour JF, Schattenberg JM, Kawaguchi T, Arrese M, Valenti L, Shiha G, Tiribelli C, Yki-Järvinen H, Fan JG, Grønbæk H, Yilmaz Y, Cortez-Pinto H, Oliveira CP, Bedossa P, Adams LA, Zheng MH, Fouad Y, Chan WK, Mendez-Sanchez N, Ahn SH, Castera L, Bugianesi E, Ratziu V, George J. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J Hepatol. 2020;73:202–209. - PubMed
-
- Estes C, Anstee QM, Arias-Loste MT, Bantel H, Bellentani S, Caballeria J, Colombo M, Craxi A, Crespo J, Day CP, Eguchi Y, Geier A, Kondili LA, Kroy DC, Lazarus JV, Loomba R, Manns MP, Marchesini G, Nakajima A, Negro F, Petta S, Ratziu V, Romero-Gomez M, Sanyal A, Schattenberg JM, Tacke F, Tanaka J, Trautwein C, Wei L, Zeuzem S, Razavi H. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016-2030. J Hepatol. 2018;69:896–904. - PubMed
-
- Younossi ZM, Blissett D, Blissett R, Henry L, Stepanova M, Younossi Y, Racila A, Hunt S, Beckerman R. The economic and clinical burden of nonalcoholic fatty liver disease in the United States and Europe. Hepatology. 2016;64:1577–1586. - PubMed
-
- Wong RJ, Aguilar M, Cheung R, Perumpail RB, Harrison SA, Younossi ZM, Ahmed A. Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting liver transplantation in the United States. Gastroenterology. 2015;148:547–555. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
