

Skene's glands abscess an overlooked diagnosis in acute lower urinary symptoms
- PMID: 34630812
- PMCID: PMC8493500
- DOI: 10.1016/j.radcr.2021.09.006
Skene's glands abscess an overlooked diagnosis in acute lower urinary symptoms
Erratum in
-
Erratum regarding missing patient consent statements in previously published articles.Radiol Case Rep. 2023 Feb 24;18(5):2056. doi: 10.1016/j.radcr.2023.01.086. eCollection 2023 May. Radiol Case Rep. 2023. PMID: 37069954 Free PMC article.
Abstract
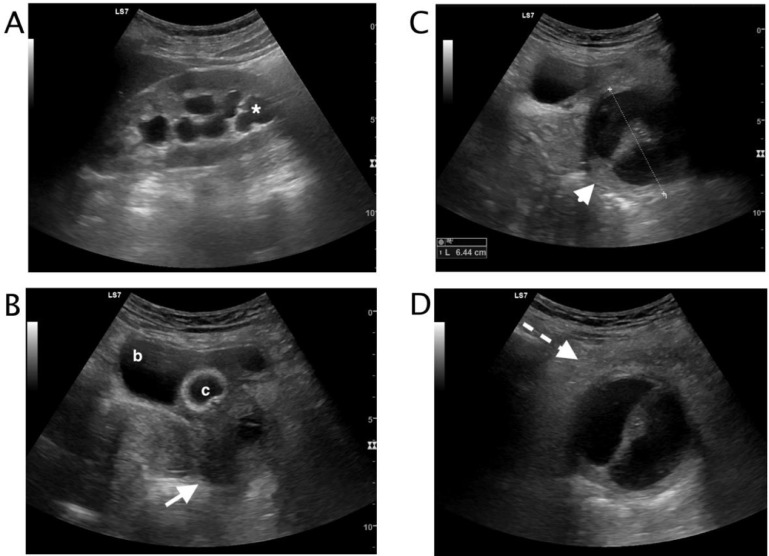
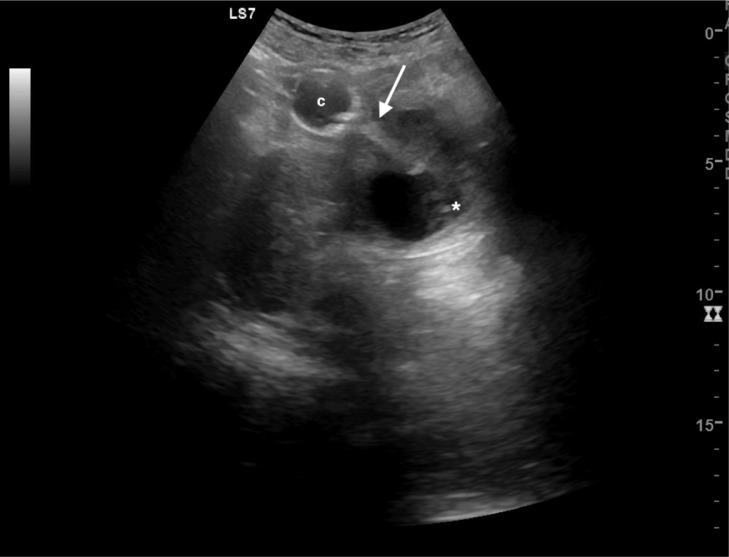
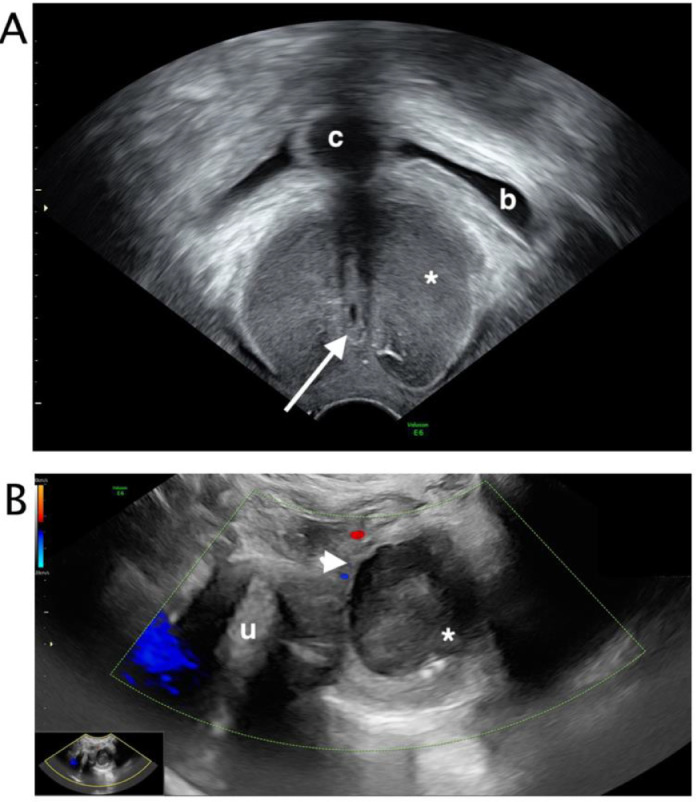
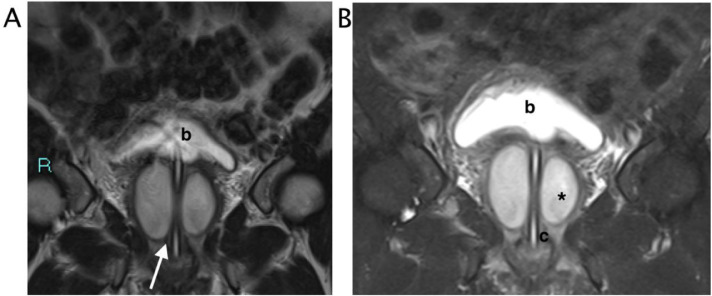
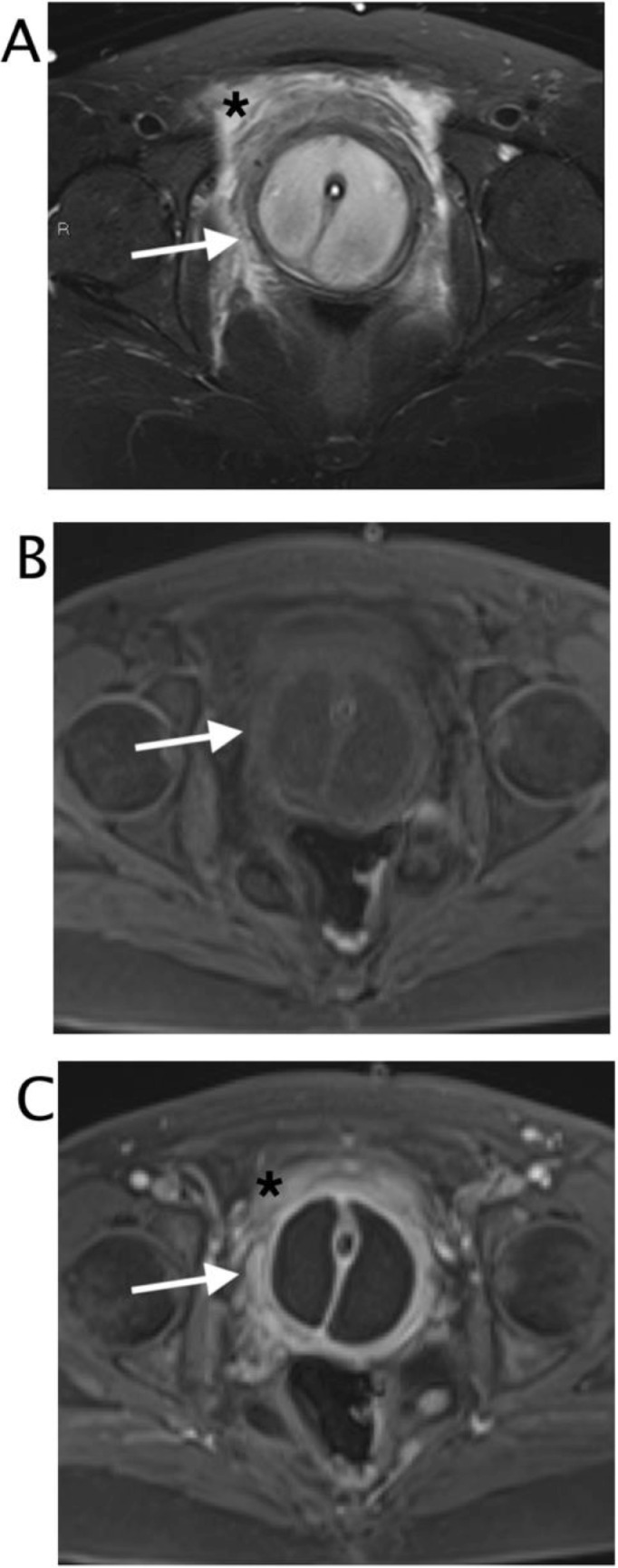
Skenitis refers to the infection of the Skene's glands. Skene's glands are paraurethral glands localized on the upper wall of the vagina. The diagnosis of Skene's glands abscess or infection is usually made based on the history and physical examination, but half of women with para-urethral gland symptoms present with non-palpable lesions and necessitate further evaluation with imaging. Patients may present with chronic urethral pain, recurrent urinary tract infections, unexplained dyspareunia, and dysuria. At imaging Skene's glands are typically located on the anterior vaginal wall, at symphysis level and paramedian to urethra. Clinicians should consider Skenitis in the differential diagnosis of lower urinary tract symptoms. We report a case of a 48-year-old woman with acute lower urinary tract symptoms with a final diagnosis of Skene's glands abscess.
Keywords: Lower urinary tract symptoms; MRI; Magnetic Resonance Imaging; Paraurethral abscess; Skene's glands abscess; Skenitis; ULTRASOUND; US; paraurethral glands.
© 2021 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures
Similar articles
-
[First results of using the original urethral speculum for diagnosing chronic skenitis].Urologiia. 2024 Nov;(5):65-70. Urologiia. 2024. PMID: 39564845 Russian.
-
Adenosquamous Carcinoma of Skene's Gland: A Case Report and Literature Review.Front Oncol. 2022 Aug 9;12:893980. doi: 10.3389/fonc.2022.893980. eCollection 2022. Front Oncol. 2022. PMID: 36016628 Free PMC article.
-
Skene's gland cyst excision.Int Urogynecol J. 2016 May;27(5):817-20. doi: 10.1007/s00192-015-2872-9. Epub 2015 Dec 15. Int Urogynecol J. 2016. PMID: 26670578
-
Skene's gland adenocarcinoma with intestinal differentiation: A case report and literature review.Pathol Int. 2017 Nov;67(11):575-579. doi: 10.1111/pin.12571. Epub 2017 Sep 5. Pathol Int. 2017. PMID: 28872768 Review.
-
Skene's Gland Malignancy: A Case Report and Systematic Review.Urology. 2022 Jul;165:36-43. doi: 10.1016/j.urology.2022.02.004. Epub 2022 Feb 19. Urology. 2022. PMID: 35192863
Cited by
-
Lesser vestibular periurethral gland-like inflammation associated with lower urinary tract signs in a female dog.J Vet Intern Med. 2023 Nov-Dec;37(6):2488-2491. doi: 10.1111/jvim.16889. Epub 2023 Sep 29. J Vet Intern Med. 2023. PMID: 37772480 Free PMC article.
-
Large Cyst of Skene Gland: A Rare Perineum Mass.Surg J (N Y). 2023 May 14;9(2):e71-e74. doi: 10.1055/s-0043-1768944. eCollection 2023 Apr. Surg J (N Y). 2023. PMID: 37192958 Free PMC article.
References
-
- Heller D.S. Lesions of Skene glands and periurethral region: a review. J Low Genit Tract Dis. 2015;19(2):170–174. - PubMed
-
- CM Desmarais. Skene's Gland Abscess: Detection With Transperineal Sonography. J of Diagnostic Med Sonog. 2015;31:390–393.
-
- Bennett G.L., Hecht E.M., Tanpitukpongse T.P., Babb J.S., Taouli B., Wong S. MRI of the urethra in women with lower urinary tract symptoms: spectrum of findings at static and dynamic imaging. AJR Am J Roentgenol. 2009;193(6):1708–1715. - PubMed
-
- Blaivas J.G. Periurethral masses: etiology and diagnosis in a large series of women. Obstet Gynecol. 2004;103(5 Pt 1):842–847. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
