

A Scoping Review of the Evidence regarding Assessment and Management of Psychological Features of Shoulder Pain
- PMID: 34631168
- PMCID: PMC8497138
- DOI: 10.1155/2021/7211201
A Scoping Review of the Evidence regarding Assessment and Management of Psychological Features of Shoulder Pain
Abstract
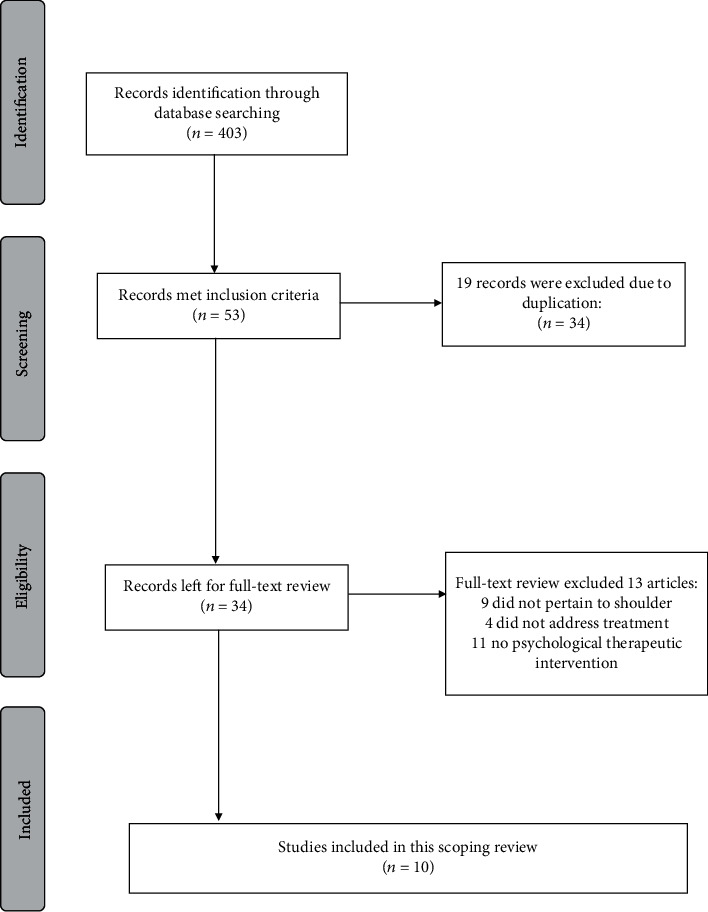
Methods: A scoping review of research studies identified through PubMed, EMBASE, and CINAHL and graduate theses identified using Google Scholar was conducted to determine studies and systematic reviews that addressed the management of psychological aspects of shoulder pain with or without neck pain. The search terms included psychological factors, anxiety, depression, catastrophic thinking, fear of movement, and psychological treatments. Two investigators screened study titles and abstracts. Data extraction, content analysis, and thematic coding focused on the dimensions of pain addressed (emotional, behavioural, and cognitive) and treatment approaches used (dimensions targeted, specific treatment parameters) and the linkage between treatment targets/rationale with interventions/outcomes measured.
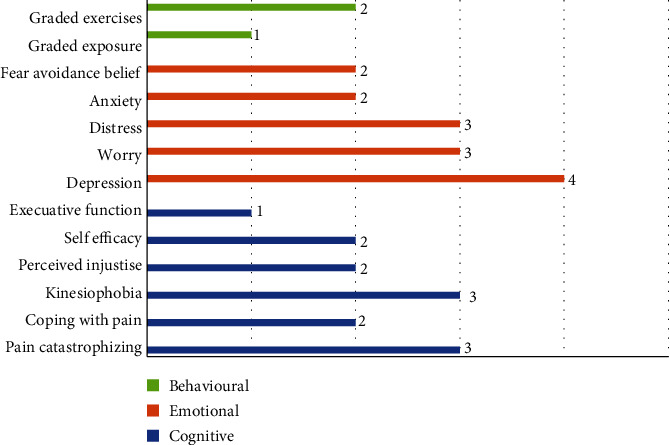
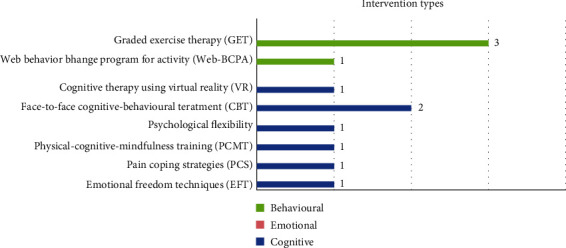
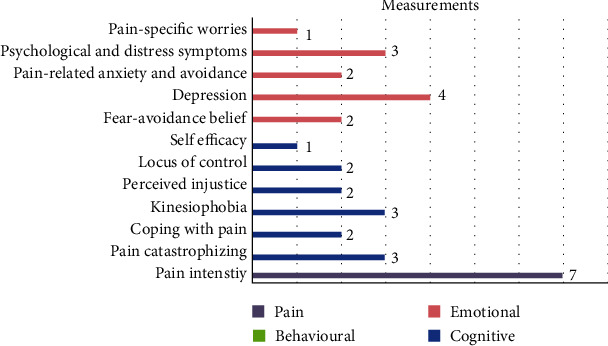
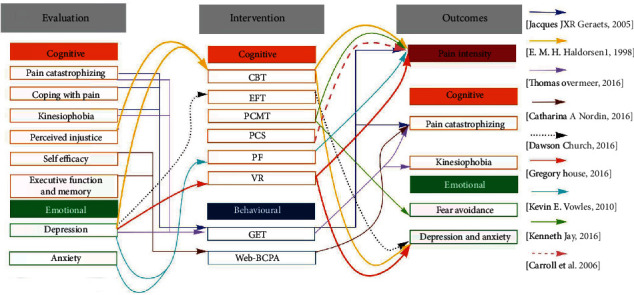
Results: Ten studies (seven randomized trials and three cohorts) were identified that addressed the psychological aspects of shoulder pain. Out of seven RCTs, four compared psychological interventions with usual care. Eight studies used cognitive approaches, including emotional freedom techniques (EFT), pain coping strategies (PCS), physical-cognitive-mindfulness training (PCMT), psychological flexibility, face-to-face cognitive-behavioural treatment (CBT), and cognitive therapy using virtual reality (V.R.). Three studies used the behavioural approaches as their intervention, including behavioural therapy and Graded Exercise Therapy (GET). Pain intensity was addressed as the primary outcome in two studies and as a secondary outcome in five studies. Cognitive factors were evaluated in 50% of the articles using nine different measures. Emotional factors were evaluated in 80% of articles using ten different measures. Reduction of pain intensity and catastrophic thinking concerning pain was achieved in most studies using a biopsychosocial approach (70%). Applying a behavioural approach was associated with reductions in kinesiophobia and pain catastrophizing. Cognitive approaches had a positive association with reductions in the emotional aspect of pain. Only one study specifically linked rationale or specific physical and psychosocial treatment targets with the treatments provided and outcomes measured.
Conclusions: Small pools of studies indicate that the rationale and treatment targeting are poorly defined in biopsychosocial interventions for shoulder pain. However, these benefits have been demonstrated when cognitive or behavioural components are added to the standard physical treatment of shoulder pain. A better definition of treatment targets, description of intervention components, and linkage of outcomes to targets are needed to advance our understanding of optimizing bio-psychosocial approaches.
Copyright © 2021 Maryam Farzad et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Behavioural modification interventions for medically unexplained symptoms in primary care: systematic reviews and economic evaluation.Health Technol Assess. 2020 Sep;24(46):1-490. doi: 10.3310/hta24460. Health Technol Assess. 2020. PMID: 32975190 Free PMC article.
-
The effect of exercise therapy combined with psychological therapy on physical activity and quality of life in patients with painful diabetic neuropathy: a systematic review.Scand J Pain. 2019 Jul 26;19(3):433-439. doi: 10.1515/sjpain-2019-0001. Scand J Pain. 2019. PMID: 31112511
-
Behavioural interventions for type 2 diabetes: an evidence-based analysis.Ont Health Technol Assess Ser. 2009;9(21):1-45. Epub 2009 Oct 1. Ont Health Technol Assess Ser. 2009. PMID: 23074526 Free PMC article.
-
Telephone interventions for symptom management in adults with cancer.Cochrane Database Syst Rev. 2020 Jun 2;6(6):CD007568. doi: 10.1002/14651858.CD007568.pub2. Cochrane Database Syst Rev. 2020. PMID: 32483832 Free PMC article.
-
Psychosocial interventions for preventing and treating depression in dialysis patients.Cochrane Database Syst Rev. 2019 Dec 2;12(12):CD004542. doi: 10.1002/14651858.CD004542.pub3. Cochrane Database Syst Rev. 2019. PMID: 31789430 Free PMC article.
Cited by
-
Physical Therapist Management of Glenohumeral Joint Osteoarthritis: A Clinical Practice Guideline from the American Physical Therapy Association.Phys Ther. 2023 Jun 5;103(6):pzad041. doi: 10.1093/ptj/pzad041. Phys Ther. 2023. PMID: 37115808 Free PMC article.
-
Same patient but different worlds: A state-of-the-art review translating best practice psychosocial care from musculoskeletal care to the orthopaedic context.BMC Musculoskelet Disord. 2024 Dec 5;25(1):998. doi: 10.1186/s12891-024-08107-4. BMC Musculoskelet Disord. 2024. PMID: 39639261 Free PMC article. Review.
-
Perspectives of North American firefighters on navigating interventions and healthcare choices for work-related shoulder disorders.Discov Public Health. 2025;22(1):342. doi: 10.1186/s12982-025-00739-8. Epub 2025 Jun 16. Discov Public Health. 2025. PMID: 40534899 Free PMC article.
References
-
- Özkan S., Zale E. L., Ring D., Vranceanu A.-M. Associations between pain catastrophizing and cognitive fusion in relation to pain and upper extremity function among hand and upper extremity surgery patients. Annals of Behavioral Medicine . 2017;51(4):547–554. doi: 10.1007/s12160-017-9877-1. - DOI - PubMed
-
- MacDermid J. C., Valdes K., Szekeres M., Naughton N., Algar L. The assessment of psychological factors on upper extremity disability: a scoping review. Journal of Hand Therapy . 2018;31:511–523. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
