

A Prediction Model of Extubation Failure Risk in Preterm Infants
- PMID: 34631610
- PMCID: PMC8492984
- DOI: 10.3389/fped.2021.693320
A Prediction Model of Extubation Failure Risk in Preterm Infants
Abstract
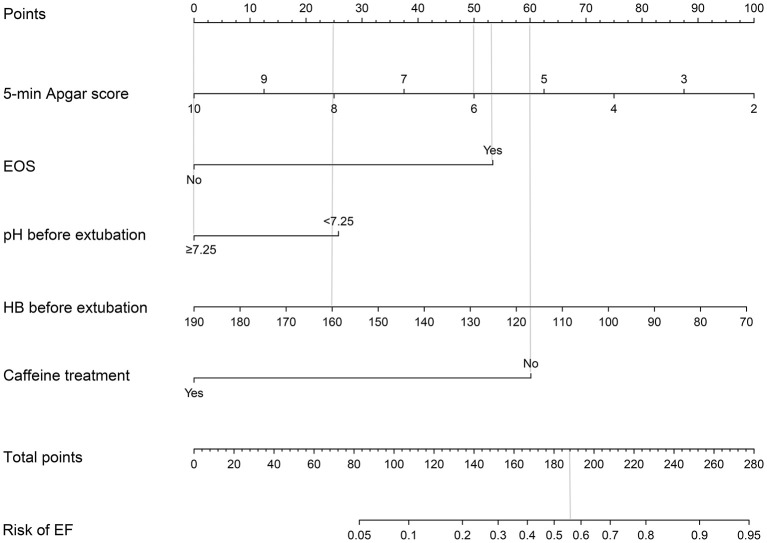
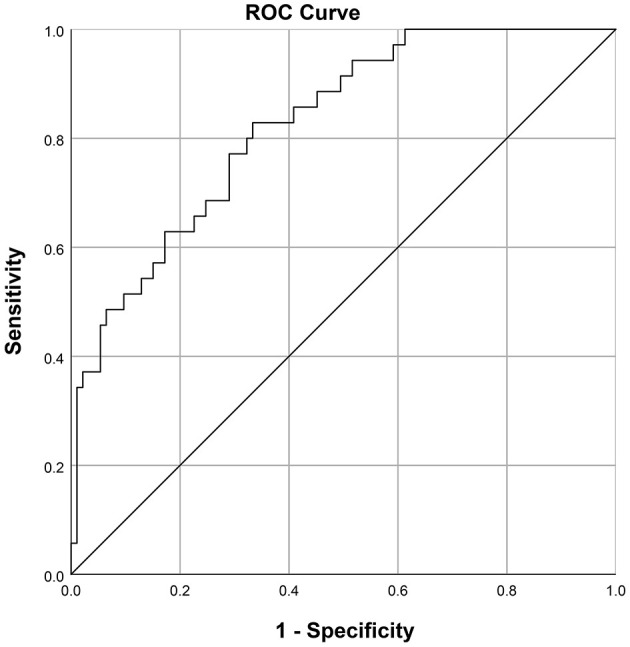
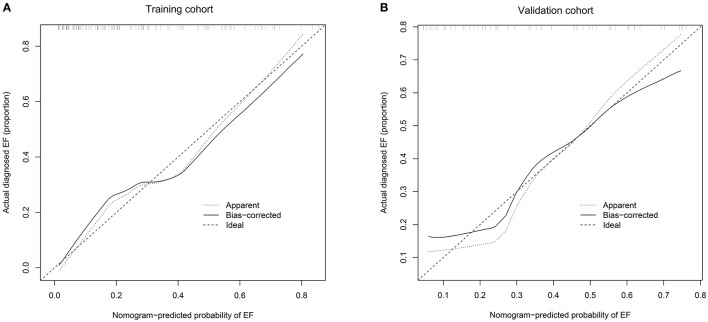
Objectives: This study aimed to identify variables and develop a prediction model that could estimate extubation failure (EF) in preterm infants. Study Design: We enrolled 128 neonates as a training cohort and 58 neonates as a validation cohort. They were born between 2015 and 2020, had a gestational age between 250/7 and 296/7 weeks, and had been treated with mechanical ventilation through endotracheal intubation (MVEI) because of acute respiratory distress syndrome. In the training cohort, we performed univariate logistic regression analysis along with stepwise discriminant analysis to identify EF predictors. A monogram based on five predictors was built. The concordance index and calibration plot were used to assess the efficiency of the nomogram in the training and validation cohorts. Results: The results of this study identified a 5-min Apgar score, early-onset sepsis, hemoglobin before extubation, pH before extubation, and caffeine administration as independent risk factors that could be combined for accurate prediction of EF. The EF nomogram was created using these five predictors. The area under the receiver operator characteristic curve was 0.824 (95% confidence interval 0.748-0.900). The concordance index in the training and validation cohorts was 0.824 and 0.797, respectively. The calibration plots showed high coherence between the predicted probability of EF and actual observation. Conclusions: This EF nomogram was a useful model for the precise prediction of EF risk in preterm infants who were between 250/7 and 296/7 weeks' gestational age and treated with MVEI because of acute respiratory distress syndrome.
Keywords: early-onset sepsis; extubation; hemoglobin; mechanical ventilation; preterm infant.
Copyright © 2021 Cheng, Dong, Zhao, Zhang, Han, Gong and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A nomogram to predict extubation failure in infants born before 32 gestational weeks: a single-center retrospective study.Transl Pediatr. 2025 May 30;14(5):776-787. doi: 10.21037/tp-2025-43. Epub 2025 May 27. Transl Pediatr. 2025. PMID: 40519731 Free PMC article.
-
A Nomogram for Predicting Extubation Failure in Preterm Infants with Gestational Age Less than 29 Weeks.Neonatology. 2023;120(4):424-433. doi: 10.1159/000530759. Epub 2023 May 31. Neonatology. 2023. PMID: 37257426
-
A prediction nomogram for neonatal acute respiratory distress syndrome in late-preterm infants and full-term infants: A retrospective study.EClinicalMedicine. 2022 Jun 25;50:101523. doi: 10.1016/j.eclinm.2022.101523. eCollection 2022 Aug. EClinicalMedicine. 2022. PMID: 35784441 Free PMC article.
-
A prediction nomogram for moderate-to-severe bronchopulmonary dysplasia in preterm infants < 32 weeks of gestation: A multicenter retrospective study.Front Pediatr. 2023 Apr 3;11:1102878. doi: 10.3389/fped.2023.1102878. eCollection 2023. Front Pediatr. 2023. PMID: 37077339 Free PMC article.
-
Advancing necrotizing enterocolitis prediction through iterative monitoring.Transl Pediatr. 2024 May 31;13(5):770-783. doi: 10.21037/tp-24-15. Epub 2024 May 20. Transl Pediatr. 2024. PMID: 38840675 Free PMC article.
Cited by
-
Risk Factors for Extubation Failure After Pediatric Cardiac Surgery and Impact on Outcomes: A Multicenter Analysis.Crit Care Explor. 2023 Sep 22;5(10):e0966. doi: 10.1097/CCE.0000000000000966. eCollection 2023 Oct. Crit Care Explor. 2023. PMID: 37753236 Free PMC article.
-
Predictors of successful extubation from volume-targeted ventilation in extremely preterm neonates.J Perinatol. 2024 Feb;44(2):250-256. doi: 10.1038/s41372-023-01849-4. Epub 2023 Dec 20. J Perinatol. 2024. PMID: 38123799
-
Development of a clinical prediction tool for extubation failure in pediatric cardiac intensive care unit.Front Pediatr. 2024 Mar 5;12:1346198. doi: 10.3389/fped.2024.1346198. eCollection 2024. Front Pediatr. 2024. PMID: 38504995 Free PMC article.
-
Predictors of extubation failure in newborns: a systematic review and meta-analysis.Ital J Pediatr. 2023 Oct 2;49(1):133. doi: 10.1186/s13052-023-01538-0. Ital J Pediatr. 2023. PMID: 37784184 Free PMC article.
-
Risk factors and adverse outcomes of extubation failure in preterm infants ≤32 weeks with neonatal respiratory distress syndrome.Front Pediatr. 2025 Jul 10;13:1555521. doi: 10.3389/fped.2025.1555521. eCollection 2025. Front Pediatr. 2025. PMID: 40708905 Free PMC article.
References
LinkOut - more resources
Full Text Sources