

Effect of Dynamic Circuit Pressures Monitoring on the Lifespan of Extracorporeal Circuit and the Efficiency of Solute Removal During Continuous Renal Replacement Therapy
- PMID: 34631725
- PMCID: PMC8494973
- DOI: 10.3389/fmed.2021.621921
Effect of Dynamic Circuit Pressures Monitoring on the Lifespan of Extracorporeal Circuit and the Efficiency of Solute Removal During Continuous Renal Replacement Therapy
Abstract
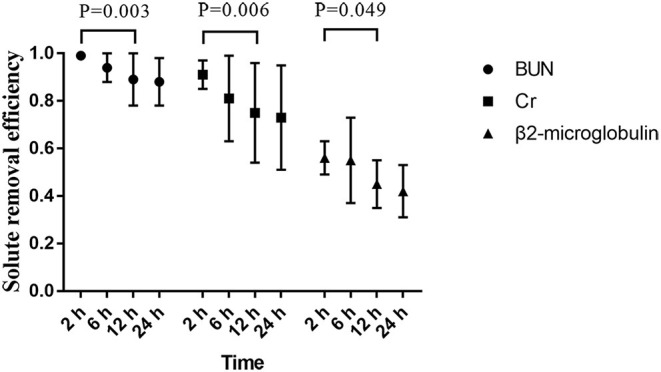
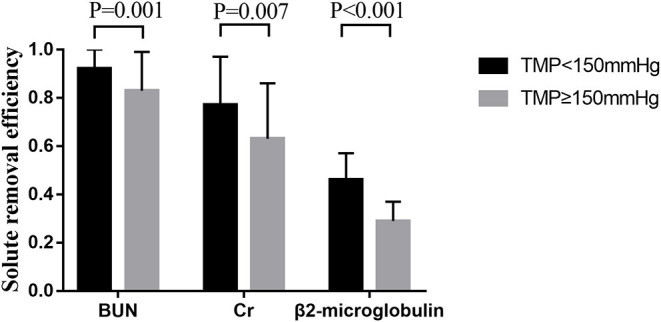
Objective: To observe the effects of dynamic pressure monitoring on the lifespan of the extracorporeal circuit and the efficiency of solute removal during continuous renal replacement therapy (CRRT). Materials and Methods: A prospective observational study was performed at the West China Hospital of Sichuan University in the ICU. Analyses of the downloaded pressure data recorded by CRRT machines and the solute removal efficiencies, calculated by 2*Ce/(Cpre+Cpost), where Ce, Cpre, and Cpost are the concentrations of the effluent, pre-filter blood, and post-filter blood, respectively, were performed. Samples were collected at 0, 2, 6, 12, and 24 h when continuous veno-venous hemodiafiltration (CVVHDF) was used after the initiation of CRRT. Measurements in concentrations of creatinine, blood urea nitrogen, and β2-microglobulin in the plasma and effluent were recorded. Results: Extracorporeal circuits characterized by moderate-to-severe (M-S) access outflow dysfunction (AOD) events, defined as access outflow pressure less than or equal to -200 mmHg for more than 5 min, had shorter median lifespans with no anticoagulation (32.3 vs. 10.90 h, P = 0.001) compared with the no M-S AOD events group. The significant outcome also existed in regional citrate anticoagulation (RCA) (72 vs. 42.47 h, P = 0.02). Moreover, Cox regression analysis revealed that the lack of M-S AOD events, RCA, or CVVHDF independently prolonged the circuit lifespan. All tested solutes removal efficiencies started to decline at 12 h. Furthermore, efficiencies of all solutes removal dropped obviously at 24 h when TMP ≥ 150 mmHg. Conclusion: RCA and CVVHDF predicted a longer circuit lifespan. M-S AOD events were associated with a shorter circuit lifespan when RCA or no anticoagulant was used. Replacement of extracorporeal circuit could be considered when running time of filter lasted up to 24 h with TMP ≥ 150 mmHg.
Keywords: access outflow dysfunction; circuit pressures; continuous renal replacement therapy; extracorporeal circuit failure; solute removal efficiency.
Copyright © 2021 Li, Zhang, Lin, Tang, Guan, Wei and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Validation of a Protocol for Continuous Hemodiafiltration with Regional Citrate Anticoagulation with Omni®.Blood Purif. 2022;51(12):1039-1047. doi: 10.1159/000524329. Epub 2022 May 30. Blood Purif. 2022. PMID: 35636389 Free PMC article.
-
Calcium-containing versus calcium-free replacement solution in regional citrate anticoagulation for continuous renal replacement therapy: a randomized controlled trial.Chin Med J (Engl). 2022 Oct 20;135(20):2478-2487. doi: 10.1097/CM9.0000000000002369. Chin Med J (Engl). 2022. PMID: 36583864 Free PMC article. Clinical Trial.
-
Complications of Regional Citrate Anticoagulation for Continuous Renal Replacement Therapy: An Observational Study.Blood Purif. 2020;49(5):567-575. doi: 10.1159/000506253. Epub 2020 Mar 3. Blood Purif. 2020. PMID: 32126564 Clinical Trial.
-
Citrate Anticoagulation during Continuous Renal Replacement Therapy.Contrib Nephrol. 2017;190:19-30. doi: 10.1159/000468833. Epub 2017 May 23. Contrib Nephrol. 2017. PMID: 28535516 Review.
-
Regional citrate anticoagulation for continuous renal replacement therapy.Curr Opin Crit Care. 2018 Dec;24(6):450-454. doi: 10.1097/MCC.0000000000000547. Curr Opin Crit Care. 2018. PMID: 30247214 Review.
Cited by
-
Development and validation of a nomogram for circuit lifespan of regional citrate anticoagulation-continuous renal replacement therapy in intensive care patients with acute kidney injury.Nurs Crit Care. 2025 Jul;30(4):e13196. doi: 10.1111/nicc.13196. Epub 2024 Nov 7. Nurs Crit Care. 2025. PMID: 39511929 Free PMC article.
-
Risk factors for unplanned weaning of continuous renal replacement therapy in ICU patients: a meta-analysis.Ren Fail. 2024 Dec;46(2):2387431. doi: 10.1080/0886022X.2024.2387431. Epub 2024 Aug 13. Ren Fail. 2024. PMID: 39135545 Free PMC article.
-
How to safeguard the continuous renal replacement therapy circuit: a narrative review.Front Med (Lausanne). 2024 Aug 21;11:1442065. doi: 10.3389/fmed.2024.1442065. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39234046 Free PMC article. Review.
References
-
- Liu C, Mao Z, Kang H, Hu J, Zhou F. Regional citrate versus heparin anticoagulation for continuous renal replacement therapy in critically ill patients: a meta-analysis with trial sequential analysis of randomized controlled trials. Crit Care. (2016) 20:144. 10.1186/s13054-016-1299-0 - DOI - PMC - PubMed
-
- Crosswell A, Brain MJ, Roodenburg O. Vascular access site influences circuit life in continuous renal replacement therapy. Crit Care Resusc. (2014) 16:127–130. - PubMed
LinkOut - more resources
Full Text Sources