

Association of Serum 25-Hydroxyvitamin D Concentrations With All-Cause and Cause-Specific Mortality Among Adult Patients With Existing Cardiovascular Disease
- PMID: 34631770
- PMCID: PMC8496747
- DOI: 10.3389/fnut.2021.740855
Association of Serum 25-Hydroxyvitamin D Concentrations With All-Cause and Cause-Specific Mortality Among Adult Patients With Existing Cardiovascular Disease
Abstract
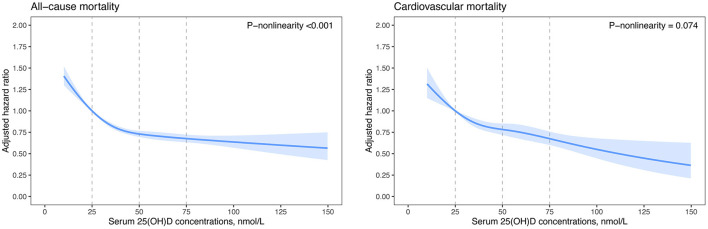
Background: Vitamin D insufficiency and deficiency are common in patients with cardiovascular disease (CVD). We aimed to prospectively examine the associations of serum 25-hydroxyvitamin D [25(OH)D] concentrations with all-cause and cause-specific mortality among adult patients with existing CVD. Methods: We included 37,079 patients with CVD from the UK Biobank study, a prospective cohort of half a million participants aged 40-69 years. We defined patients with CVD as those who suffered coronary heart disease, atrial fibrillation, heart failure, or stroke. The associations of serum 25(OH)D concentration with all-cause and cause-specific mortality were examined by using multivariable Cox regression models and competing risk analyses. Results: Among 37,079 patients with CVD at baseline, 57.5% were subjected to vitamin D deficiency (i.e., 25[OH]D <50 nmol/L). During a median follow-up of 11.7 years, 6,319 total deaths occurred, including 2,161 deaths from CVD, 2,230 deaths from cancer, 623 deaths from respiratory disease, and 1,305 other-cause deaths. We observed non-linear inverse associations for all-cause, cancer, respiratory disease, and other-cause mortality (P-non-linearity <0.01) and approximately linear inverse associations for CVD mortality (P-non-linearity = 0.074). Among CVD patients with vitamin D deficiency, per 10 nmol/L increment in serum 25(OH)D concentrations was associated with an 12% reduced risk for all-cause mortality and 9% reduced risk for CVD mortality. Conclusion: Among patients with existing CVD, increasing levels in serum 25(OH)D were independently associated with a decreased risk of all-cause and cause-specific mortality. These findings suggest that elevated serum 25(OH)D concentration benefits CVD patients with vitamin D deficiency.
Keywords: UK Biobank; cardiovascular disease; cohort study; mortality; vitamin D.
Copyright © 2021 Dai, Liu and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Associations of serum 25-hydroxyvitamin D and vitamin D receptor polymorphisms with risks of cardiovascular disease and mortality among patients with chronic kidney disease: a prospective study.Am J Clin Nutr. 2024 Jun;119(6):1397-1404. doi: 10.1016/j.ajcnut.2024.04.001. Epub 2024 Apr 10. Am J Clin Nutr. 2024. PMID: 38608754
-
Estimating dose-response relationships for vitamin D with coronary heart disease, stroke, and all-cause mortality: observational and Mendelian randomisation analyses.Lancet Diabetes Endocrinol. 2021 Dec;9(12):837-846. doi: 10.1016/S2213-8587(21)00263-1. Epub 2021 Oct 28. Lancet Diabetes Endocrinol. 2021. Retraction in: Lancet Diabetes Endocrinol. 2024 Jan;12(1):8. doi: 10.1016/S2213-8587(23)00364-9. Retracted and republished in: Lancet Diabetes Endocrinol. 2024 Jan;12(1):e2-e11. doi: 10.1016/S2213-8587(23)00287-5. PMID: 34717822 Free PMC article. Retracted. Retracted and republished.
-
L-shaped association of serum 25-hydroxyvitamin D concentrations with cardiovascular and all-cause mortality in individuals with osteoarthritis: results from the NHANES database prospective cohort study.BMC Med. 2022 Sep 21;20(1):308. doi: 10.1186/s12916-022-02510-1. BMC Med. 2022. PMID: 36127705 Free PMC article.
-
Circulating 25-hydroxy-vitamin D and risk of cardiovascular disease: a meta-analysis of prospective studies.Circ Cardiovasc Qual Outcomes. 2012 Nov;5(6):819-29. doi: 10.1161/CIRCOUTCOMES.112.967604. Epub 2012 Nov 13. Circ Cardiovasc Qual Outcomes. 2012. PMID: 23149428 Free PMC article. Review.
-
Serum 25(OH)D Concentration, Vitamin D Supplementation, and Risk of Cardiovascular Disease and Mortality in Patients with Type 2 Diabetes or Prediabetes: a Systematic Review and Dose-Response Meta-Analysis.Am J Clin Nutr. 2023 Sep;118(3):697-707. doi: 10.1016/j.ajcnut.2023.07.012. Epub 2023 Jul 18. Am J Clin Nutr. 2023. PMID: 37467897
Cited by
-
Life's essential 8 and risk of all-cause mortality in individuals with cardiovascular diseases: A prospective community-based study.Clin Cardiol. 2024 Feb;47(2):e24119. doi: 10.1002/clc.24119. Epub 2023 Nov 23. Clin Cardiol. 2024. PMID: 37994466 Free PMC article.
-
Neutrophil-to-Lymphocyte Ratio Is Not Associated with Severity of Coronary Artery Disease and Is Not Correlated with Vitamin D Level in Patients with a History of an Acute Coronary Syndrome.Biology (Basel). 2022 Jul 1;11(7):1001. doi: 10.3390/biology11071001. Biology (Basel). 2022. PMID: 36101382 Free PMC article.
-
Higher Vitamin D Levels before Methotrexate Therapy Initiation Are Associated with Lower Subsequent Mortality in Patients with Rheumatoid Arthritis.Nutrients. 2024 Jan 30;16(3):401. doi: 10.3390/nu16030401. Nutrients. 2024. PMID: 38337687 Free PMC article.
-
The Role of Exercise-Induced Molecular Processes and Vitamin D in Improving Cardiorespiratory Fitness and Cardiac Rehabilitation in Patients With Heart Failure.Front Physiol. 2022 Jan 11;12:794641. doi: 10.3389/fphys.2021.794641. eCollection 2021. Front Physiol. 2022. PMID: 35087418 Free PMC article. Review.
-
Higher Serum 25-Hydroxyvitamin D Is Associated with Lower All-Cause and Cardiovascular Mortality among US Adults with Nonalcoholic Fatty Liver Disease.Nutrients. 2022 Sep 27;14(19):4013. doi: 10.3390/nu14194013. Nutrients. 2022. PMID: 36235666 Free PMC article.
References
-
- GBD 2017 Causes of Death Collaborators . Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1736–88. 10.1016/S0140-6736(18)32203-7 - DOI - PMC - PubMed
-
- Lutsey PL, Michos ED, Misialek JR, Pankow JS, Loehr L, Selvin E, et al. . Race and vitamin D binding protein gene polymorphisms modify the association of 25-hydroxyvitamin D and incident heart failure: the ARIC (Atherosclerosis Risk in Communities) study. JACC Heart Fail. (2015) 3:347–56. 10.1016/j.jchf.2014.11.013 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources