

Prediction of Recurrent Atrial Tachyarrhythmia After Receiving Atrial Flutter Ablation in Patients With Prior Cardiac Surgery for Valvular Heart Disease
- PMID: 34631838
- PMCID: PMC8495322
- DOI: 10.3389/fcvm.2021.741377
Prediction of Recurrent Atrial Tachyarrhythmia After Receiving Atrial Flutter Ablation in Patients With Prior Cardiac Surgery for Valvular Heart Disease
Abstract
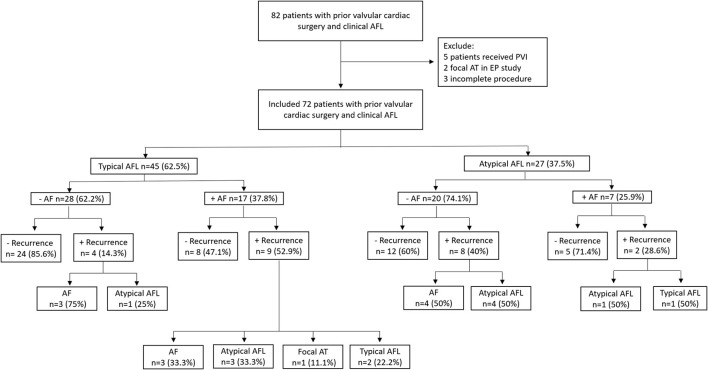
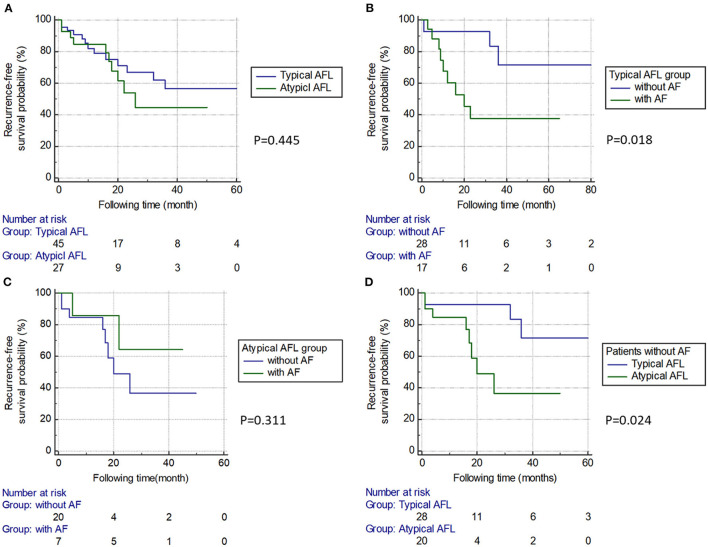
Background: Surgical scars cause an intra-atrial conduction delay and anatomical obstacles that facilitate the perpetuation of atrial flutter (AFL). This study aimed to investigate the outcome and predictor of recurrent atrial tachyarrhythmia after catheter ablation in patients with prior cardiac surgery for valvular heart disease (VHD) who presented with AFL. Methods: Seventy-two patients with prior cardiac surgery for VHD who underwent AFL ablation were included. The patients were categorized into a typical AFL group (n = 45) and an atypical AFL group (n = 27). The endpoint was the recurrence of atrial tachyarrhythmia during follow-up. A multivariate analysis was performed to determine the predictor of recurrence. Results: No significant difference was found in the recurrence rate of atrial tachyarrhythmia between the two groups. Patients with concomitant atrial fibrillation (AF) had a higher recurrence of typical AFL compared with those without AF (13 vs. 0%, P = 0.012). In subgroup analysis, typical AFL patients with concomitant AF had a higher incidence of recurrent atrial tachyarrhythmia than those without it (53 vs. 14%, P = 0.006). Regarding patients without AF, the typical AFL group had a lower recurrence rate of atrial tachyarrhythmia than the atypical AFL group (14 vs. 40%, P = 0.043). Multivariate analysis showed that chronic kidney disease (CKD) and left atrial diameter (LAD) were independent predictors of recurrence. Conclusions: In our study cohort, concomitant AF was associated with recurrence of atrial tachyarrhythmia. CKD and LAD independently predicted recurrence after AFL ablation in patients who have undergone cardiac surgery for VHD.
Keywords: ablation; atrial fibrillation; atrial flutter; heart surgery; valvular heart disease.
Copyright © 2021 Chou, Chung, Chang, Lin, Lo, Hu, Chao, Liao, Tuan, Lin, Chang, Liu, Wu, Huang, Chen, Cheng, Liu, Lugtu, Jain, Feng, Chang and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Recurrent atrial flutter and atrial fibrillation after catheter ablation of the cavotricuspid isthmus: a very long-term follow-up of 333 patients.J Interv Card Electrophysiol. 2002 Dec;7(3):225-31. doi: 10.1023/a:1021392105994. J Interv Card Electrophysiol. 2002. PMID: 12510133
-
Higher rate of recurrent atrial flutter and atrial fibrillation following atrial flutter ablation after cardiac surgery.J Cardiovasc Electrophysiol. 2010 Jul;21(7):760-5. doi: 10.1111/j.1540-8167.2009.01709.x. Epub 2010 Feb 1. J Cardiovasc Electrophysiol. 2010. PMID: 20132385
-
Ablation outcomes for atypical atrial flutter versus recurrent atrial fibrillation following index pulmonary vein isolation.J Cardiovasc Electrophysiol. 2021 Jun;32(6):1631-1639. doi: 10.1111/jce.15051. Epub 2021 May 5. J Cardiovasc Electrophysiol. 2021. PMID: 33928697
-
Cavotricuspid isthmus line in patients undergoing catheter ablation of atrial fibrillation with or without history of typical atrial flutter: A meta-analysis.J Cardiovasc Electrophysiol. 2020 Aug;31(8):1987-1995. doi: 10.1111/jce.14614. Epub 2020 Jul 7. J Cardiovasc Electrophysiol. 2020. PMID: 32530541
-
Atrial fibrillation inducibility during cavotricuspid isthmus-dependent atrial flutter ablation as a predictor of clinical atrial fibrillation. A meta-analysis.J Interv Card Electrophysiol. 2017 Apr;48(3):307-315. doi: 10.1007/s10840-016-0211-9. Epub 2017 Jan 9. J Interv Card Electrophysiol. 2017. PMID: 28070875 Review.
Cited by
-
Electrophysiological characteristics of epicardial breakthrough during catheter ablation of perimitral atrial flutter.Front Cardiovasc Med. 2022 Nov 17;9:1030916. doi: 10.3389/fcvm.2022.1030916. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36465473 Free PMC article.
References
-
- Nakagawa H, Shah N, Matsudaira K, Overholt E, Chandrasekaran K, Beckman KJ, et al. . Characterization of reentrant circuit in macroreentrant right atrial tachycardia after surgical repair of congenital heart disease: isolated channels between scars allow “focal” ablation. Circulation. (2001) 103:699–709. 10.1161/01.CIR.103.5.699 - DOI - PubMed
LinkOut - more resources
Full Text Sources