

The Injured Shoulder in High-Level Male Gymnasts, Part 1: Epidemiology and Pathoanatomy of Surgically Treated Lesions
- PMID: 34631906
- PMCID: PMC8493315
- DOI: 10.1177/23259671211043449
The Injured Shoulder in High-Level Male Gymnasts, Part 1: Epidemiology and Pathoanatomy of Surgically Treated Lesions
Abstract
Background: Weightbearing and traction-suspension movements with the upper limbs put considerable demands upon the shoulder region of high-level gymnasts. The diagnosis of instability in these gymnasts may be difficult because voluntary inferior shoulder subluxation is part of their training and is needed to perform some acrobatic figures.
Purpose: To (1) assess the epidemiology of shoulder lesions requiring surgery, (2) describe the types of injuries and assess which maneuvers and equipment put the gymnast most at risk, and (3) present a pathoanatomic classification of the injured shoulder in high-level male gymnasts.
Study design: Case series; Level of evidence, 4.
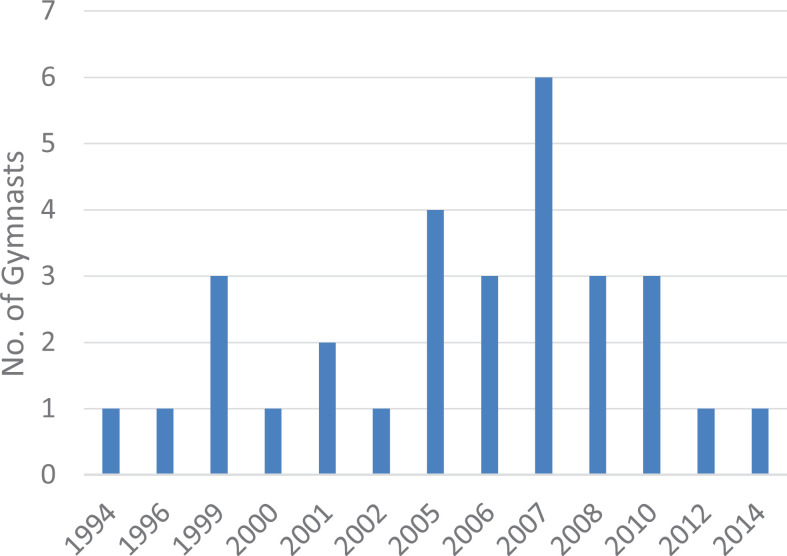
Methods: Over a 20-year period (1994-2014), 26 high-level male gymnasts (30 shoulders; mean age, 22 years; range, 16-33 years) were referred to our surgical center for shoulder pain or instability. Four gymnasts underwent surgery on both shoulders. All shoulders were evaluated clinically, radiologically, and arthroscopically. An independent observer evaluated the circumstances in which these lesions occurred, including the apparatus used and the maneuvers performed.
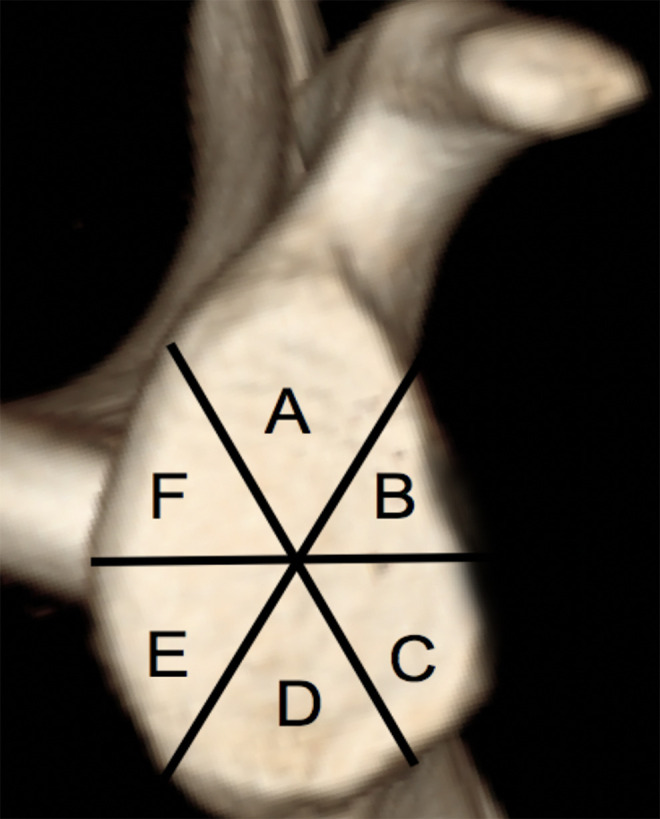
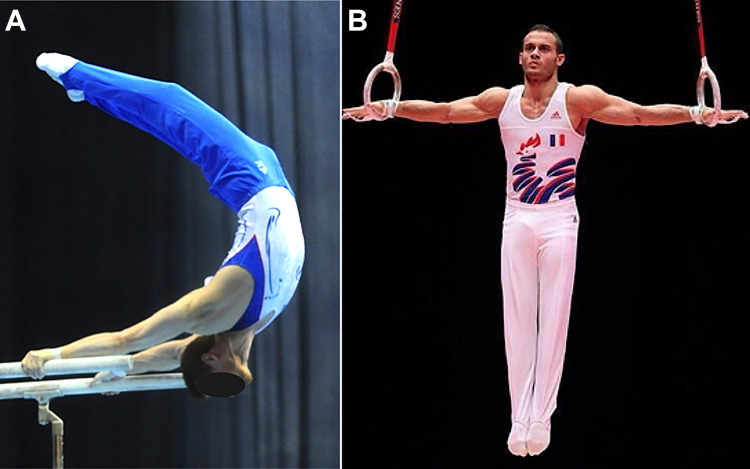
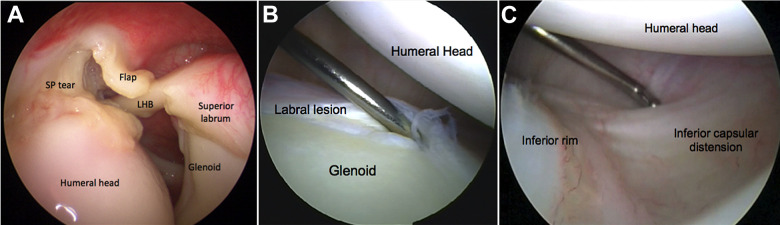
Results: The mean duration of symptoms before surgery was 8 months (range, 6-24 months). Eighteen injured shoulders (60%) had chronic overuse injuries. In 27 shoulders (90%), the mechanism of injury was traction of the arm in forced flexion-rotation while using suspension equipment with locked hands on the bars or the rings. In the remaining 3 shoulders, the traumatic position was one of an isometric muscle contraction against gravity, sustained while performing strength-and-hold positions on the rings. Based on the main presenting symptoms (pain and/or instability) and main anatomic lesions found during arthroscopy, the injured gymnasts' shoulders were classified into 2 categories: painful shoulders (n = 13) with no clinical, radiological, or arthroscopic findings of instability (mainly superior cuff and biceps anchor lesions) and unstable shoulders (n = 17) with isolated inferior capsule labral tears or mixed lesions (tendinous and capsulolabral). Some gymnasts with inferior labral tears had no recall of having suffered a dislocation or subluxation.
Conclusion: The majority of injuries requiring surgery in this population occurred during traction in forced flexion-rotation using suspension equipment. Injured shoulders were classified as either painful or unstable shoulders.
Keywords: SLAP lesions; high-level gymnasts; instability; labral tears; partial cuff tears; shoulder arthroscopy; shoulder injury.
© The Author(s) 2021.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: P.B. has received consulting fees from Smith & Nephew and royalties from Tornier/Wright. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
Similar articles
-
The Injured Shoulder in High-Level Male Gymnasts, Part 2: Can Athletes Return to Competition After Surgery?Orthop J Sports Med. 2021 Oct 4;9(10):23259671211043468. doi: 10.1177/23259671211043468. eCollection 2021 Oct. Orthop J Sports Med. 2021. PMID: 34631907 Free PMC article.
-
Superior Labral Injuries in Elite Gymnasts: Symptoms, Pathology, and Outcomes After Surgical Repair.Orthop J Sports Med. 2020 Jul 14;8(7):2325967120935001. doi: 10.1177/2325967120935001. eCollection 2020 Jul. Orthop J Sports Med. 2020. PMID: 32704508 Free PMC article.
-
Lesions of the biceps pulley.Am J Sports Med. 2011 Apr;39(4):790-5. doi: 10.1177/0363546510393942. Epub 2011 Feb 18. Am J Sports Med. 2011. PMID: 21335355
-
[Arthroscopic stabilization of the shoulder with suture anchors with special reference to the deep anterior-inferior portal (5.30 o'clock)].Oper Orthop Traumatol. 2007 Jun;19(2):133-54. doi: 10.1007/s00064-007-1199-1. Oper Orthop Traumatol. 2007. PMID: 17530195 Review. German.
-
[The gymnastics shoulder].Orthopade. 2014 Mar;43(3):230-5. doi: 10.1007/s00132-013-2145-6. Orthopade. 2014. PMID: 24604156 Review. German.
Cited by
-
Relationship Between Bench Press and Iron Cross Maximal Isometric Contraction-How to Develop the Strength to Perform the Iron Cross on Rings.Eur J Sport Sci. 2025 Jul;25(7):e70002. doi: 10.1002/ejsc.70002. Eur J Sport Sci. 2025. PMID: 40638591 Free PMC article. Clinical Trial.
-
Effectiveness of a sport-specific exercise programme for overhead athletes with unilateral subacromial shoulder pain: a study protocol of a randomised controlled trial.BMJ Open Sport Exerc Med. 2025 Mar 13;11(1):e002523. doi: 10.1136/bmjsem-2025-002523. eCollection 2025. BMJ Open Sport Exerc Med. 2025. PMID: 40092169 Free PMC article.
-
Return to Sport and Patient-Reported Outcomes After Subpectoral Biceps Tenodesis for SLAP Tear in Collegiate Gymnasts.Orthop J Sports Med. 2023 May 3;11(5):23259671231159354. doi: 10.1177/23259671231159354. eCollection 2023 May. Orthop J Sports Med. 2023. PMID: 37152551 Free PMC article.
-
The Injured Shoulder in High-Level Male Gymnasts, Part 2: Can Athletes Return to Competition After Surgery?Orthop J Sports Med. 2021 Oct 4;9(10):23259671211043468. doi: 10.1177/23259671211043468. eCollection 2021 Oct. Orthop J Sports Med. 2021. PMID: 34631907 Free PMC article.
-
Surgical Treatment of Shoulder Pathologies in Professional Gymnasts: Findings, Treatment, and Clinical Outcomes.J Clin Med. 2024 Apr 10;13(8):2183. doi: 10.3390/jcm13082183. J Clin Med. 2024. PMID: 38673456 Free PMC article.
References
-
- Aronen JG. Problems of the upper extremity in gymnastics. Clin Sports Med. 1985;4(1):61–71. - PubMed
-
- Bernasconi S, Tordi N, Parratte B, Rouillon JD, Monnier G. Surface electromyography of nine shoulder muscles in two iron cross conditions in gymnastics. J Sports Med Phys Fitness. 2004;44(3):240–245. - PubMed
-
- Bernasconi SM, Tordi NR, Parratte BM, Rouillon JD. Can shoulder muscle coordination during the support scale at ring height be replicated during training exercises in gymnastics? J Strength Cond Res. 2009;23(8):2381–2388. - PubMed
-
- Boileau P, Lafosse L.Évaluation arthroscopique et prospective des lésions d’instabilité antérieure chronique de l’épaule. In: Perspectives en arthroscopie. Springer Verlag; 2002:194–196.
-
- Boileau P, Zumstein M, Balg F, Penington S, Bicknell RT. The unstable painful shoulder (UPS) as a cause of pain from unrecognized anteroinferior instability in the young athlete. J Shoulder Elbow Surg. 2011;20(1):98–106. - PubMed
LinkOut - more resources
Full Text Sources
