

Long-Term (7-Year) Clinical Implications of Newly Unveiled Asymptomatic Abnormal Ankle-Brachial Index in Patients With Coronary Artery Disease
- PMID: 34632785
- PMCID: PMC8751871
- DOI: 10.1161/JAHA.121.021587
Long-Term (7-Year) Clinical Implications of Newly Unveiled Asymptomatic Abnormal Ankle-Brachial Index in Patients With Coronary Artery Disease
Abstract
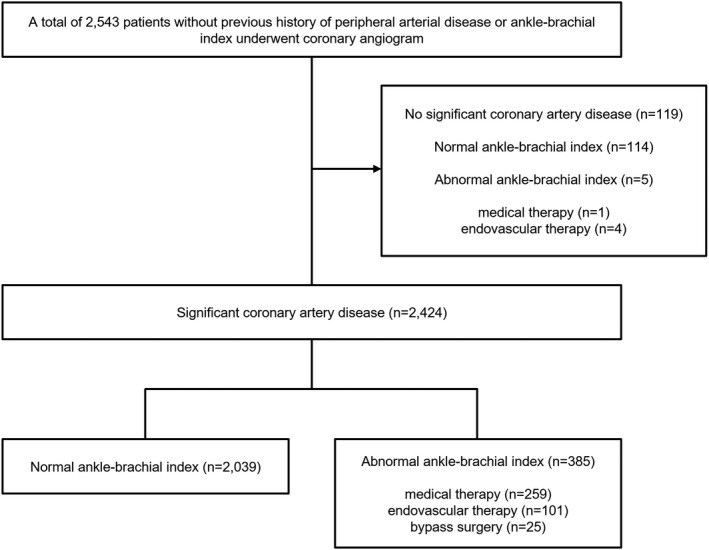
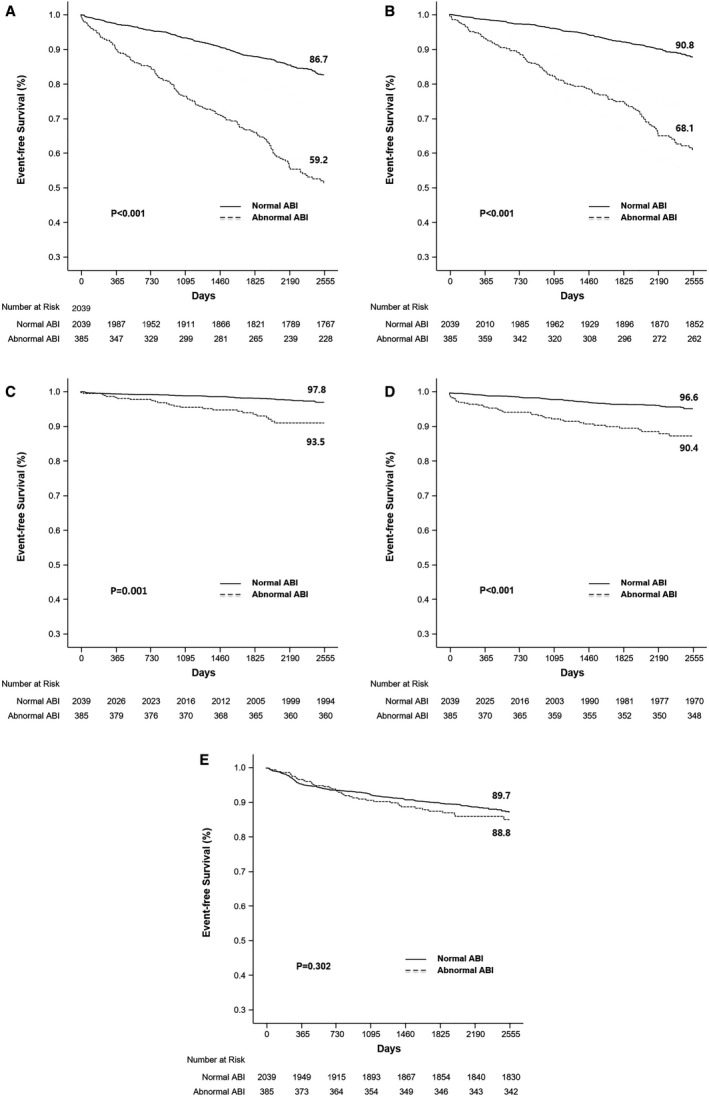
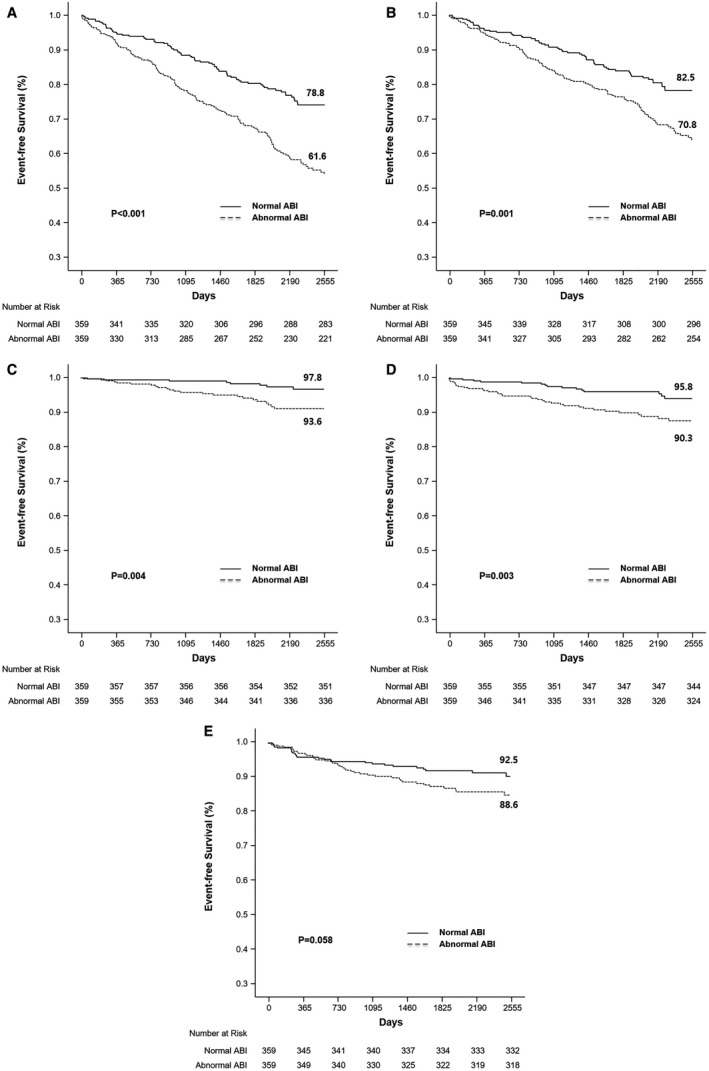
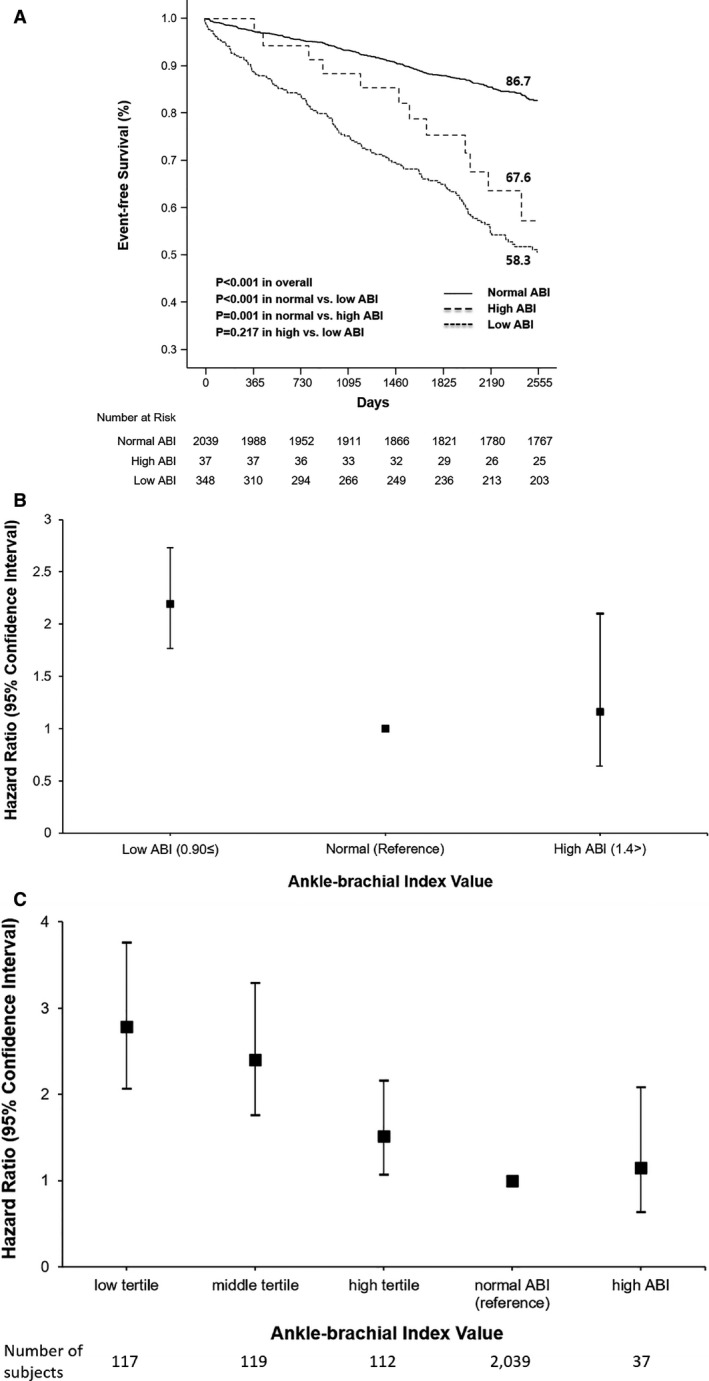
Background The long-term impact of newly discovered, asymptomatic abnormal ankle-brachial index (ABI) in patients with significant coronary artery disease is limited. Methods and Results Between January 2006 and December 2009, ABI was evaluated in 2424 consecutive patients with no history of claudication or peripheral artery disease who had significant coronary artery disease. We previously reported a 3-year result; therefore, the follow-up period was extended. The primary end point was a composite of all-cause death, myocardial infarction (MI), and stroke over 7 years. Of the 2424 patients with significant coronary artery disease, 385 had an abnormal ABI (ABI ≤0.9 or ≥1.4). During the follow-up period, the rate of the primary outcome was significantly higher in the abnormal ABI group than in the normal ABI group (P<0.001). The abnormal ABI group had a significantly higher risk of composite of all-cause death/MI/stroke than the normal ABI group, after adjustment with multivariable Cox proportional hazards regression analysis (hazard ratio [HR], 2.07; 95% CI, 1.67-2.57; P<0.001) and propensity score-matched analysis (HR, 1.97; 95% CI, 1.49-2.60; P<0.001). In addition, an abnormal ABI was associated with a higher risk of all-cause death, MI, and stroke, but not repeat revascularization. Conclusions Among patients with significant coronary artery disease, asymptomatic abnormal ABI was associated with sustained and increased incidence of composite of all-cause death/MI/stroke, all-cause death, MI, and stroke during extended follow-up over 7 years.
Keywords: ankle–brachial index; asymptomatic diseases; atherosclerosis; coronary artery disease.
Conflict of interest statement
None.
Figures
References
-
- Criqui MH, McClelland RL, McDermott MM, Allison MA, Blumenthal RS, Aboyans V, Ix JH, Burke GL, Liu K, Shea S. The ankle‐brachial index and incident cardiovascular events in the mesa (multi‐ethnic study of atherosclerosis). J Am Coll Cardiol. 2010;56:1506–1512. doi: 10.1016/j.jacc.2010.04.060. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
