

Effect of Antithrombotic Therapy on Clinical Outcomes in Outpatients With Clinically Stable Symptomatic COVID-19: The ACTIV-4B Randomized Clinical Trial
- PMID: 34633405
- PMCID: PMC8506296
- DOI: 10.1001/jama.2021.17272
Effect of Antithrombotic Therapy on Clinical Outcomes in Outpatients With Clinically Stable Symptomatic COVID-19: The ACTIV-4B Randomized Clinical Trial
Abstract
Importance: Acutely ill inpatients with COVID-19 typically receive antithrombotic therapy, although the risks and benefits of this intervention among outpatients with COVID-19 have not been established.
Objective: To assess whether anticoagulant or antiplatelet therapy can safely reduce major adverse cardiopulmonary outcomes among symptomatic but clinically stable outpatients with COVID-19.
Design, setting, and participants: The ACTIV-4B Outpatient Thrombosis Prevention Trial was designed as a minimal-contact, adaptive, randomized, double-blind, placebo-controlled trial to compare anticoagulant and antiplatelet therapy among 7000 symptomatic but clinically stable outpatients with COVID-19. The trial was conducted at 52 US sites between September 2020 and June 2021; final follow-up was August 5, 2021. Prior to initiating treatment, participants were required to have platelet count greater than 100 000/mm3 and estimated glomerular filtration rate greater than 30 mL/min/1.73 m2.
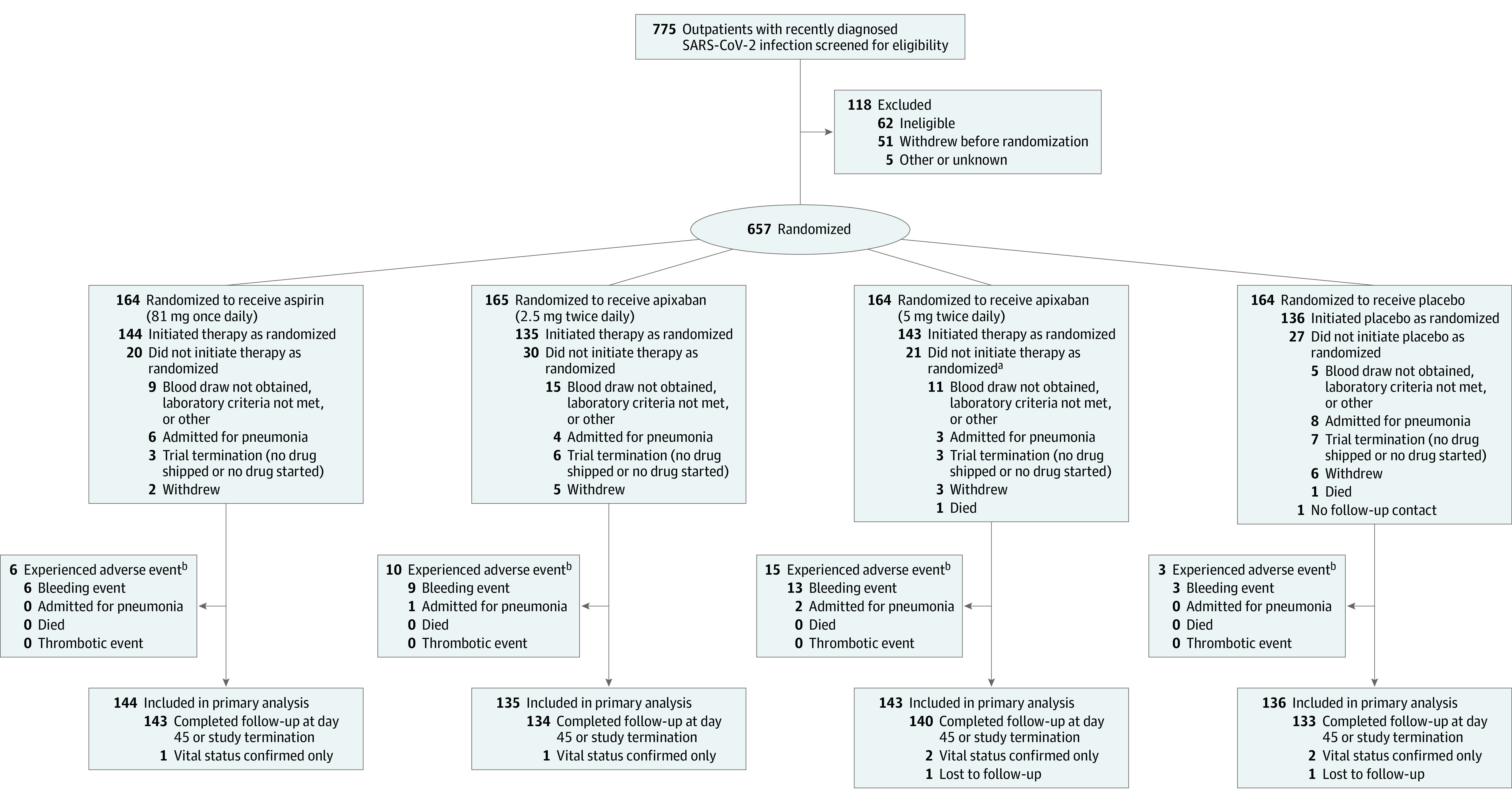
Interventions: Random allocation in a 1:1:1:1 ratio to aspirin (81 mg orally once daily; n = 164), prophylactic-dose apixaban (2.5 mg orally twice daily; n = 165), therapeutic-dose apixaban (5 mg orally twice daily; n = 164), or placebo (n = 164) for 45 days.
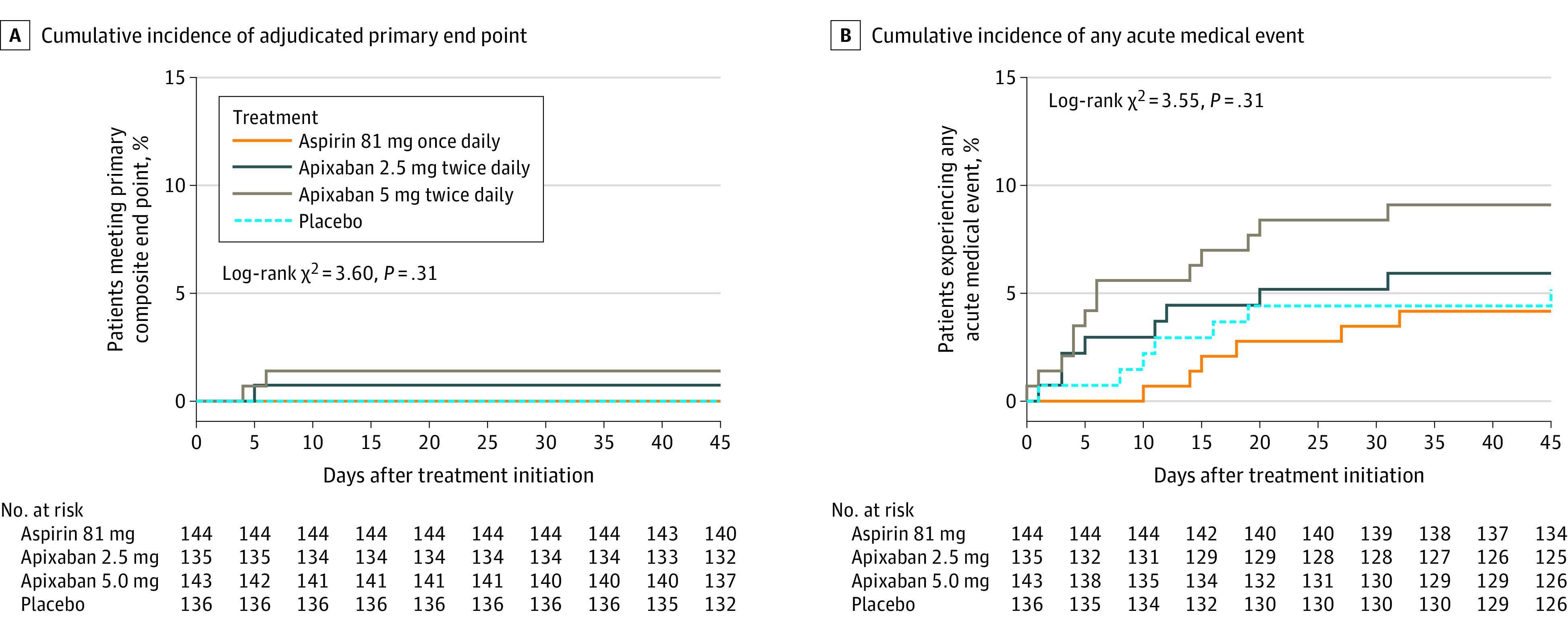
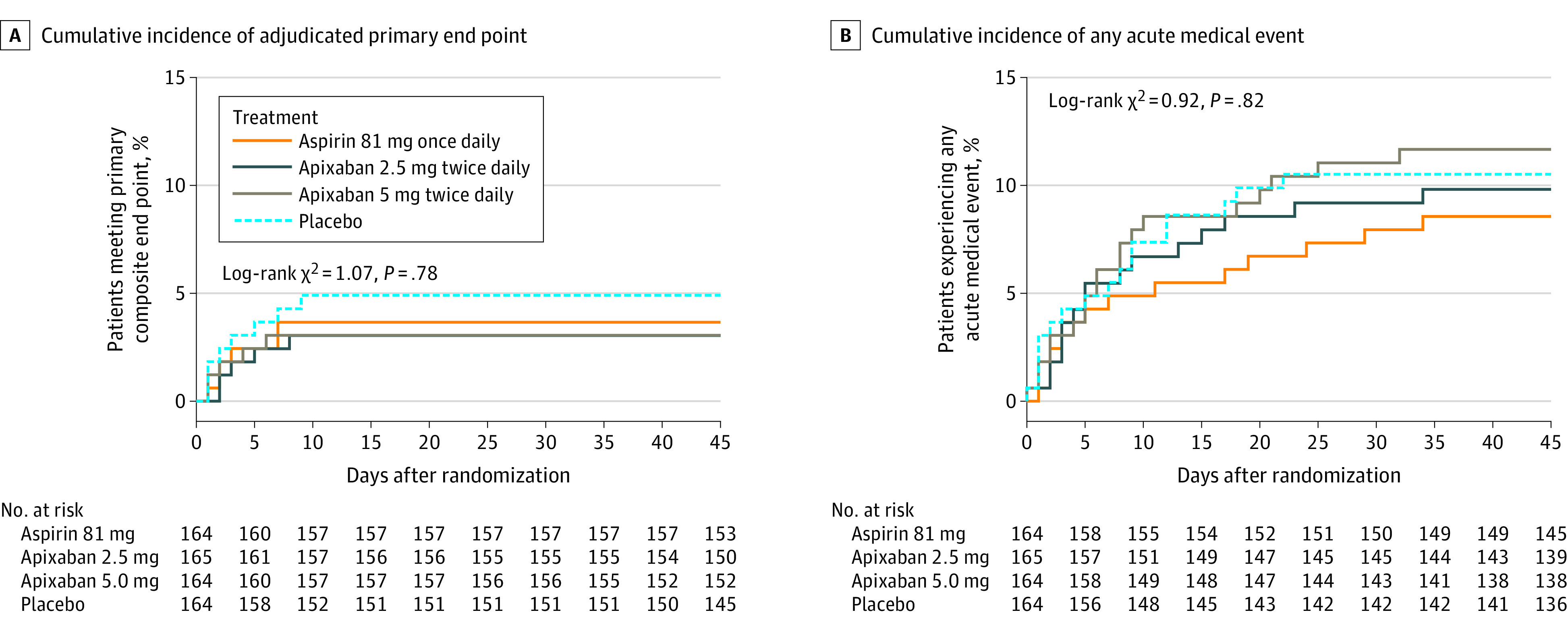
Main outcomes and measures: The primary end point was a composite of all-cause mortality, symptomatic venous or arterial thromboembolism, myocardial infarction, stroke, or hospitalization for cardiovascular or pulmonary cause. The primary analyses for efficacy and bleeding events were limited to participants who took at least 1 dose of trial medication.
Results: On June 18, 2021, the trial data and safety monitoring board recommended early termination because of lower than anticipated event rates; at that time, 657 symptomatic outpatients with COVID-19 had been randomized (median age, 54 years [IQR, 46-59]; 59% women). The median times from diagnosis to randomization and from randomization to initiation of study treatment were 7 days and 3 days, respectively. Twenty-two randomized participants (3.3%) were hospitalized for COVID-19 prior to initiating treatment. Among the 558 patients who initiated treatment, the adjudicated primary composite end point occurred in 1 patient (0.7%) in the aspirin group, 1 patient (0.7%) in the 2.5-mg apixaban group, 2 patients (1.4%) in the 5-mg apixaban group, and 1 patient (0.7%) in the placebo group. The risk differences compared with placebo for the primary end point were 0.0% (95% CI not calculable) in the aspirin group, 0.7% (95% CI, -2.1% to 4.1%) in the 2.5-mg apixaban group, and 1.4% (95% CI, -1.5% to 5.0%) in the 5-mg apixaban group. Risk differences compared with placebo for bleeding events were 2.0% (95% CI, -2.7% to 6.8%), 4.5% (95% CI, -0.7% to 10.2%), and 6.9% (95% CI, 1.4% to 12.9%) among participants who initiated therapy in the aspirin, prophylactic apixaban, and therapeutic apixaban groups, respectively, although none were major. Findings inclusive of all randomized patients were similar.
Conclusions and relevance: Among symptomatic clinically stable outpatients with COVID-19, treatment with aspirin or apixaban compared with placebo did not reduce the rate of a composite clinical outcome. However, the study was terminated after enrollment of 9% of participants because of an event rate lower than anticipated.
Trial registration: ClinicalTrials.gov Identifier: NCT04498273.
Conflict of interest statement
Figures
Comment in
-
Antithrombotic Therapy for Outpatients With COVID-19: Implications for Clinical Practice and Future Research.JAMA. 2021 Nov 2;326(17):1685-1686. doi: 10.1001/jama.2021.17460. JAMA. 2021. PMID: 34633417 No abstract available.
References
-
- Sadeghipour P, Talasaz AH, Rashidi F, et al. ; INSPIRATION Investigators . Effect of intermediate-dose vs standard-dose prophylactic anticoagulation on thrombotic events, extracorporeal membrane oxygenation treatment, or mortality among patients with COVID-19 admitted to the intensive care unit: the INSPIRATION randomized clinical trial. JAMA. 2021;325(16):1620-1630. doi: 10.1001/jama.2021.4152 - DOI - PMC - PubMed
-
- Lopes RD, de Barros E Silva PGM, Furtado RHM, et al. ; ACTION Coalition COVID-19 Brazil IV Investigators . Therapeutic versus prophylactic anticoagulation for patients admitted to hospital with COVID-19 and elevated D-dimer concentration (ACTION): an open-label, multicentre, randomised, controlled trial. Lancet. 2021;397(10291):2253-2263. doi: 10.1016/S0140-6736(21)01203-4 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
