

Using numerical modeling and simulation to assess the ethical burden in clinical trials and how it relates to the proportion of responders in a trial sample
- PMID: 34634062
- PMCID: PMC8504716
- DOI: 10.1371/journal.pone.0258093
Using numerical modeling and simulation to assess the ethical burden in clinical trials and how it relates to the proportion of responders in a trial sample
Abstract
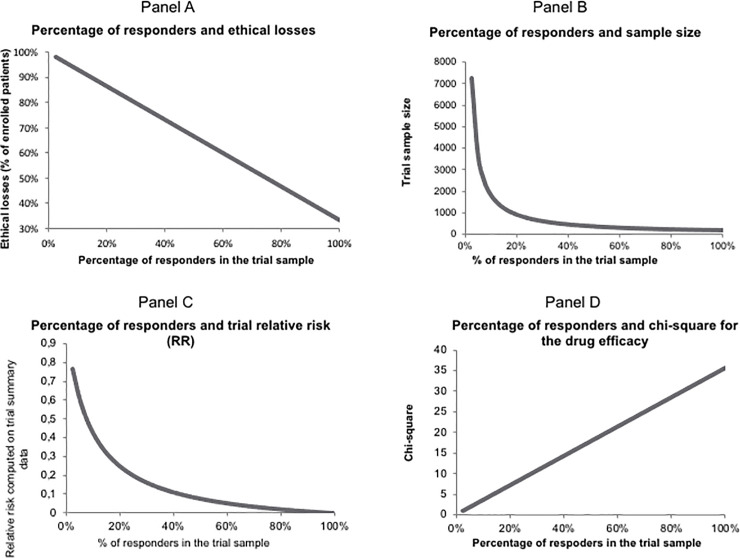
In order to propose a more precise definition and explore how to reduce ethical losses in randomized controlled clinical trials (RCTs), we set out to identify trial participants who do not contribute to demonstrating that the treatment in the experimental arm is superior to that in the control arm. RCTs emerged mid-last century as the gold standard for assessing efficacy, becoming the cornerstone of the value of new therapies, yet their ethical grounds are a matter of debate. We introduce the concept of unnecessary participants in RCTs, the sum of non-informative participants and non-responders. The non-informative participants are considered not informative with respect to the efficacy measured in the trial in contrast to responders who carry all the information required to conclude on the treatment's efficacy. The non-responders present the event whether or not they are treated with the experimental treatment. The unnecessary participants carry the burden of having to participate in a clinical trial without benefiting from it, which might include experiencing side effects. Thus, these unnecessary participants carry the ethical loss that is inherent to the RCT methodology. On the contrary, responders to the experimental treatment bear its entire efficacy in the RCT. Starting from the proportions observed in a real placebo-controlled trial from the literature, we carried out simulations of RCTs progressively increasing the proportion of responders up to 100%. We show that the number of unnecessary participants decreases steadily until the RCT's ethical loss reaches a minimum. In parallel, the trial sample size decreases (presumably its cost as well), although the trial's statistical power increases as shown by the increase of the chi-square comparing the event rates between the two arms. Thus, we expect that increasing the proportion of responders in RCTs would contribute to making them more ethically acceptable, with less false negative outcomes.
Conflict of interest statement
All authors have completed the Unified Competing Interest form (available on request from the corresponding author) and declare: no support from any organization for the submitted work [or describe if any]; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years [or describe if any], no other relationships or activities that could appear to have influenced the submitted work [or describe if any].This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Levine R, Lebacqz K. Some ethical considerations in clinical trials. Clin Pharmacol Ther. 1979;25: 728–41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
