

Kinect-based rapid movement training to improve balance recovery for stroke fall prevention: a randomized controlled trial
- PMID: 34635141
- PMCID: PMC8503723
- DOI: 10.1186/s12984-021-00922-3
Kinect-based rapid movement training to improve balance recovery for stroke fall prevention: a randomized controlled trial
Abstract
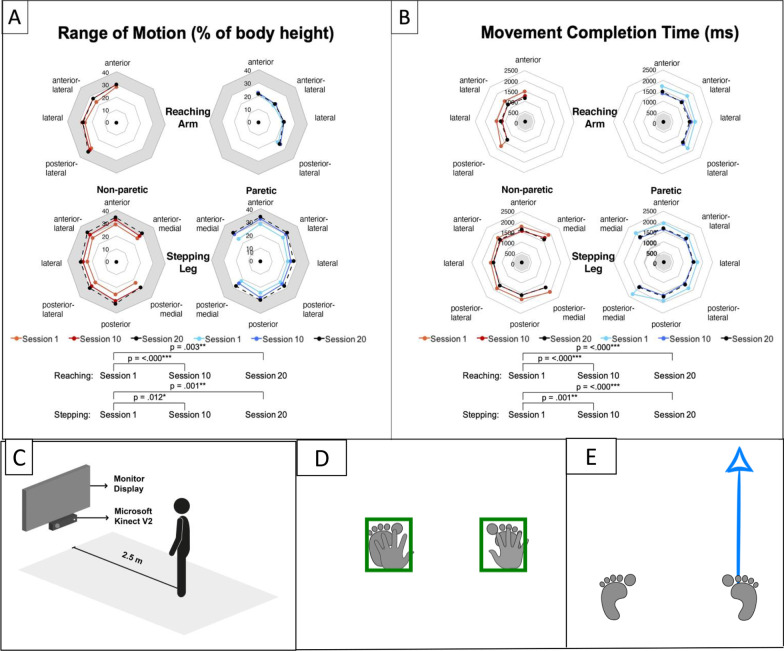
Background: Falls are more prevalent in stroke survivors than age-matched healthy older adults because of their functional impairment. Rapid balance recovery reaction with adequate range-of-motion and fast response and movement time are crucial to minimize fall risk and prevent serious injurious falls when postural disturbances occur. A Kinect-based Rapid Movement Training (RMT) program was developed to provide real-time feedback to promote faster and larger arm reaching and leg stepping distances toward targets in 22 different directions.
Objective: To evaluate the effectiveness of the interactive RMT and Conventional Balance Training (CBT) on chronic stroke survivors' overall balance and balance recovery reaction.
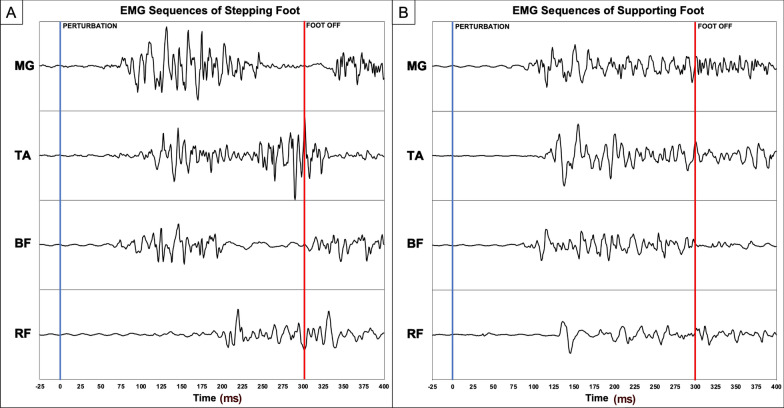
Methods: In this assessor-blinded randomized controlled trial, chronic stroke survivors were randomized to receive twenty training sessions (60-min each) of either RMT or CBT. Pre- and post-training assessments included clinical tests, as well as kinematic measurements and electromyography during simulated forward fall through a "lean-and-release" perturbation system.
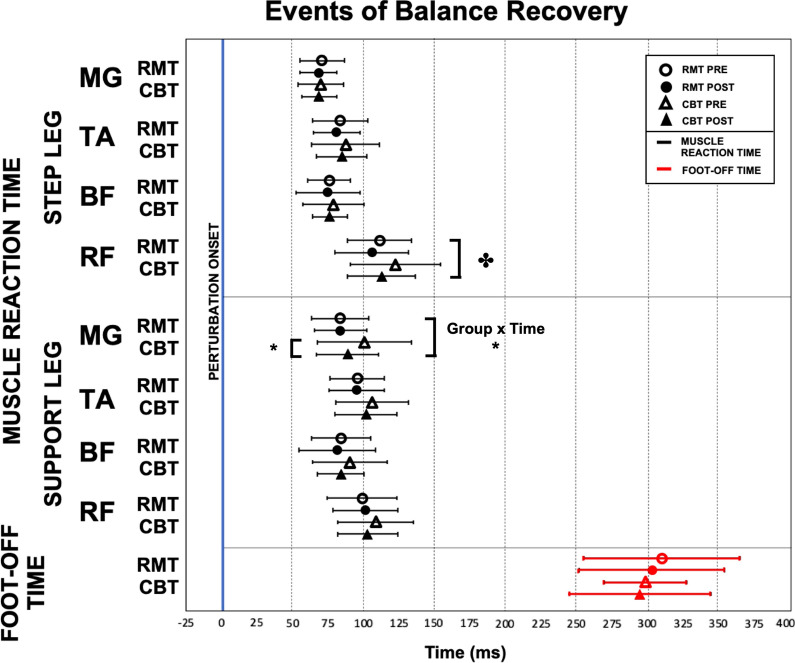
Results: Thirty participants were recruited (RMT = 16, CBT = 14). RMT led to significant improvement in balance control (Berg Balance Scale: pre = 49.13, post = 52.75; P = .001), gait control (Timed-Up-and-Go Test: pre = 14.66 s, post = 12.62 s; P = .011), and motor functions (Fugl-Meyer Assessment of Motor Recovery: pre = 60.63, post = 65.19; P = .015), which matched the effectiveness of CBT. Both groups preferred to use their non-paretic leg to take the initial step to restore stability, and their stepping leg's rectus femoris reacted significantly faster post-training (P = .036).
Conclusion: The RMT was as effective as conventional balance training to provide beneficial effects on chronic stroke survivors' overall balance, motor function and improving balance recovery with faster muscle response.
Trial registration: The study was registered at Clinicaltrials.gov ( https://clinicaltrials.gov/ct2/show/NCT03183635 , NCT03183635) on 12 June 2017.
Keywords: Balance; Falls; Posture; Slip and fall; Stroke rehabilitation; Telerehabilitation.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
