

Effect of the Emergency Department Assessment of Chest Pain Score on the Triage Performance in Patients With Chest Pain
- PMID: 34635312
- PMCID: PMC9336201
- DOI: 10.1016/j.amjcard.2021.08.058
Effect of the Emergency Department Assessment of Chest Pain Score on the Triage Performance in Patients With Chest Pain
Abstract
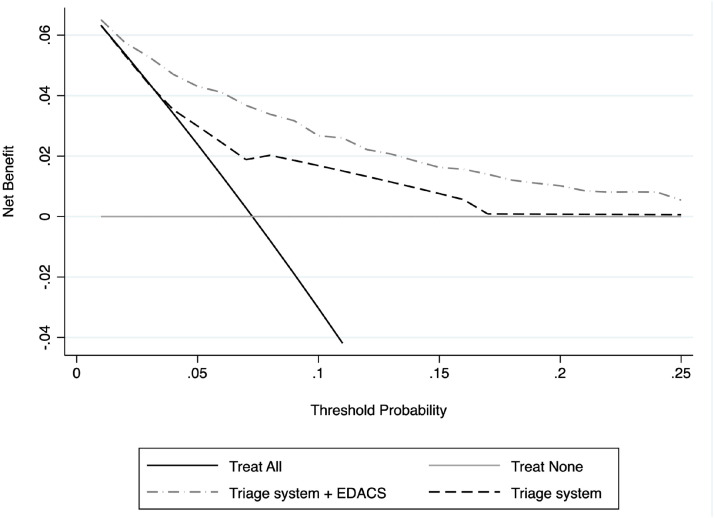
The sensitivity of triage systems in identifying acute cardiovascular events in patients presented to the emergency department with chest pain is not optimal. Recently, a clinical score, the Emergency Department Assessment of Chest Pain Score (EDACS), has been proposed for a rapid assessment without additional instruments. To evaluate whether the integration of EDACS into triage evaluation of patients with chest pain can improve the triage's predictive validity for an acute cardiovascular event, a single-center prospective observational study was conducted. This study involved all patients who needed a triage admission for chest pain between January 1, 2020, and December 31, 2020. All enrolled patients first underwent a standard triage assessment and then the EDACS was calculated. The primary outcome of the study was the presence of an acute cardiovascular event. The discriminatory ability of EDACS in triage compared with standard triage assessment was evaluated by comparing the areas under the receiver operating characteristic curve, decision curve analysis, and net reclassification improvement. The study involved 1,596 patients, of that 7.3% presented the study outcome. The discriminatory ability of triage presented an area under the receiver operating characteristic curve of 0.688 that increased to 0.818 after the application of EDACS in the triage assessment. EDACS improved the baseline assessment of priority assigned in triage, with a net reclassification improvement of 33.6% (p <0.001), and the decision curve analyses demonstrated that EDACS in triage resulted in a clear net clinical benefit. In conclusion, the results of the study suggest that EDACS has a good discriminatory capacity for acute cardiovascular events and that its implementation in routine triage may improve triage performance in patients with chest pain.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures The authors have no conflicts of interest to disclose.
Figures


References
-
- Bjørnsen LP, Naess-Pleym LE, Dale J, Grenne B, Wiseth R. Description of chest pain patients in a Norwegian emergency department. Scand Cardiovasc J. 2019;53:28–34. - PubMed
-
- Amsterdam EA, Kirk JD, Bluemke DA, Diercks D, Farkouh ME, Garvey JL, Kontos MC, McCord J, Miller TD, Morise A, Newby LK, Ruberg FL, Scordo KA, Thompson PD, American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee of the Council on Clinical Cardiology, Council on Cardiovascular Nursing, and Interdisciplinary Council on Quality of Care and Outcomes Research Testing of low-risk patients presenting to the emergency department with chest pain: a scientific statement from the American Heart Association. Circulation. 2010;122(17):1756–1776. - PMC - PubMed
-
- Chang AM, Fischman DL, Hollander JE. Evaluation of chest pain and acute coronary syndromes. Cardiol Clin. 2018;36:1–12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
