

Cost-effectiveness and system-wide impact of using Hepatitis C-viremic donors for heart transplant
- PMID: 34635381
- PMCID: PMC8973316
- DOI: 10.1016/j.healun.2021.09.002
Cost-effectiveness and system-wide impact of using Hepatitis C-viremic donors for heart transplant
Abstract
Background: The advent of direct-acting antiviral therapy for Hepatitis C (HCV) has made using HCV-viremic donors a viable strategy to address the donor shortage in heart transplantation. We employed a large-scale simulation to evaluate the impact and cost-effectiveness of using HCV-viremic donors for heart transplant.
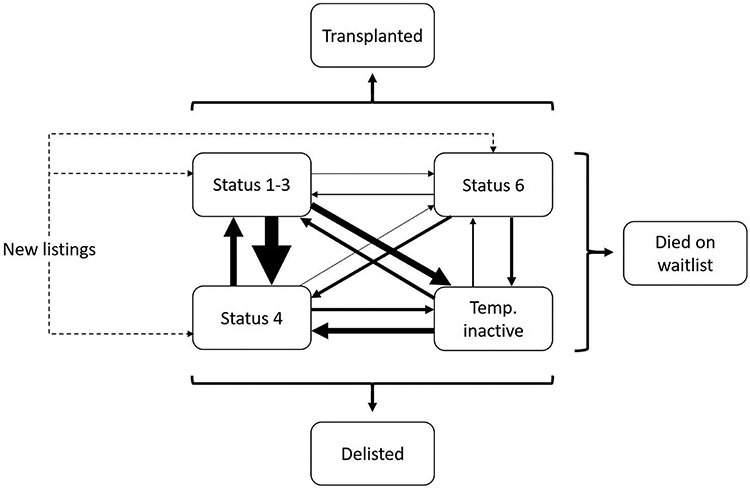
Methods: We simulated detailed histories from time of listing until death for the real-world cohort of all adults listed for heart transplant in the United States from July 2014 to June 2019 (n = 19,346). This population was imputed using historical data and captures "real-world" heterogeneity in geographic and clinical characteristics. We estimated the impact of an intervention in which all candidates accept HCV+ potential donors (n = 472) on transplant volume, waitlist outcomes, and lifetime costs and quality-adjusted life years (QALYs).
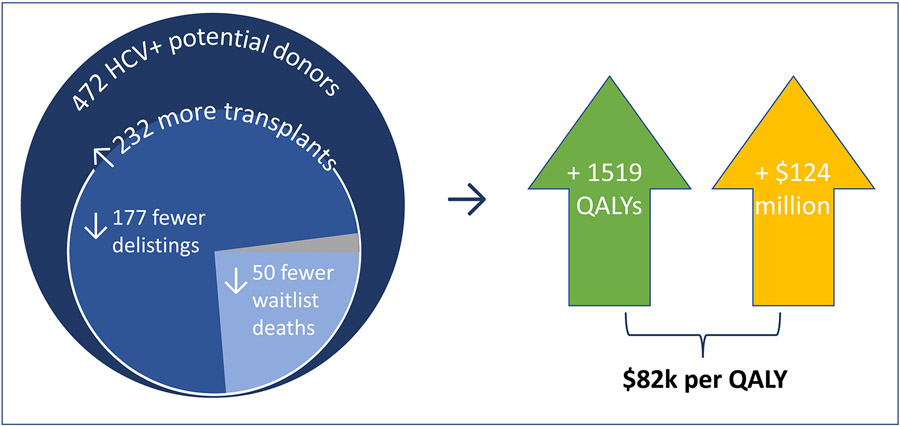
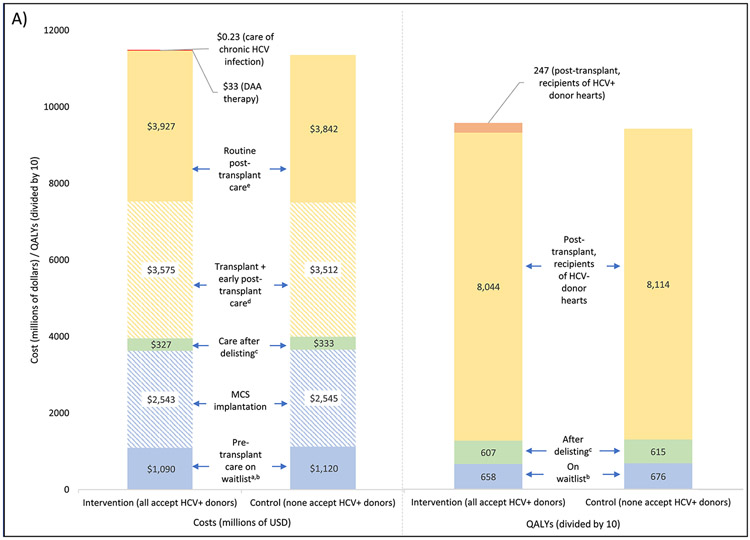
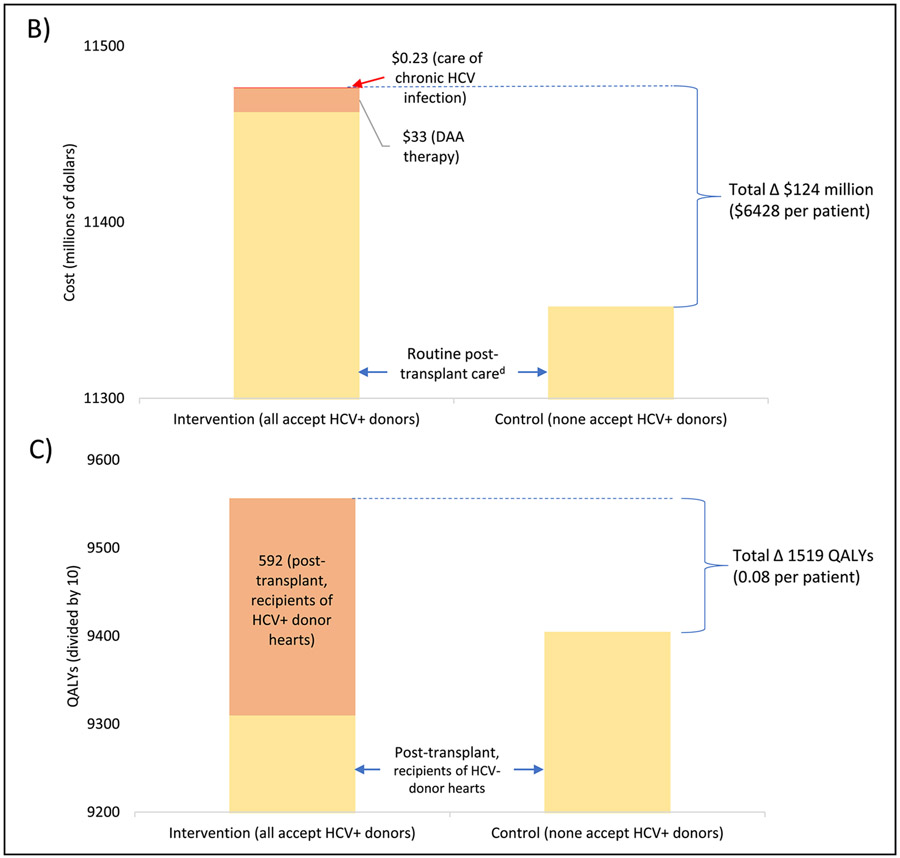
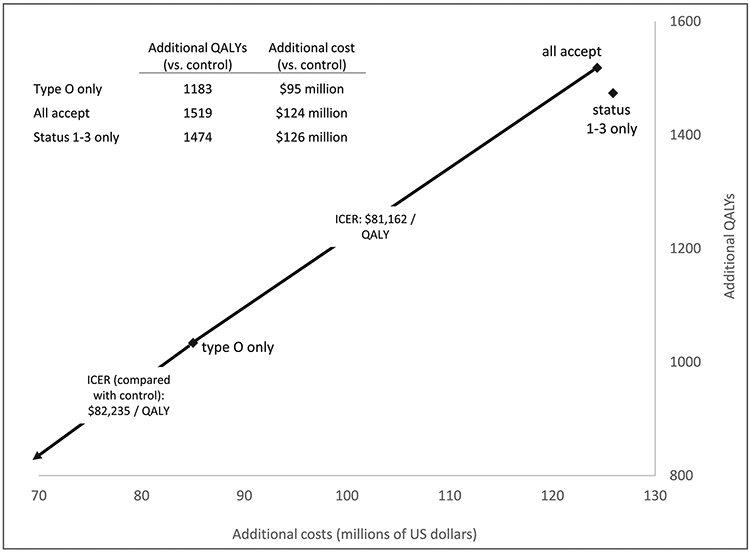
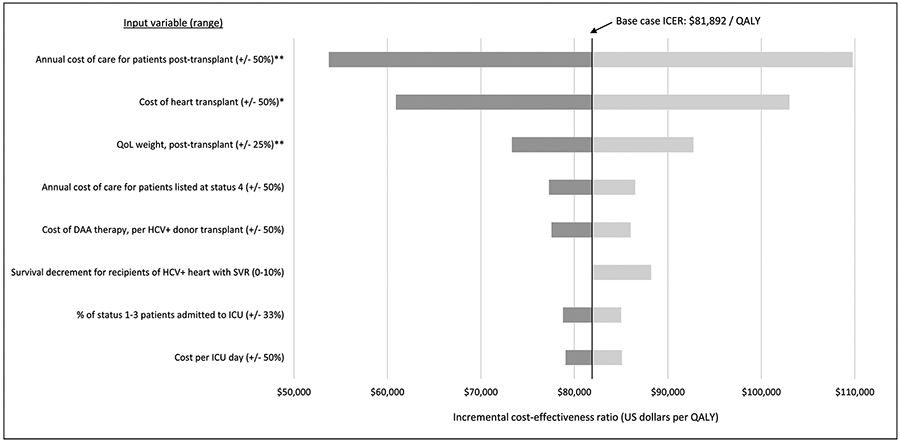
Results: The intervention produced 232 more transplants, 132 fewer delistings due to deterioration, and 50 fewer waitlist deaths within this 5-year cohort and reduced wait times by 3% to 11% (varying by priority status). The intervention was cost-effective, adding an average of 0.08 QALYs per patient at a cost of $124 million ($81,892 per QALY). DAA therapy and HCV care combined account for 11% this cost, with the remainder due to higher costs of transplant procedures and routine post-transplant care. The impact on transplant volume varied by blood type and region and was correlated with donor-to-candidate ratio (ρ = 0.71).
Conclusions: Transplanting HCV+ donor hearts is likely to be cost-effective and improve waitlist outcomes, particularly in regions and subgroups experiencing high donor scarcity.
Keywords: cost-effectiveness analysis; donor selection; health policy; heart transplantation; transplant allocation.
Copyright © 2021 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure statement Dr Teuteberg has relationships with Abbott (consulting), Abiomed (advisory board), Medtronic (speaking, advisory board), CareDx (speaking, advisory board), Paragonix (speaking). Other authors have no disclosures.
Figures
Comment in
-
Predicting the future: Hepatitis C donors in focus.J Heart Lung Transplant. 2022 Jan;41(1):48-49. doi: 10.1016/j.healun.2021.10.002. Epub 2021 Oct 22. J Heart Lung Transplant. 2022. PMID: 34802878 No abstract available.
References
-
- Cowger JA Addressing the Growing U.S. Donor Heart Shortage: Waiting for Godot or a Transplant? J Am Coll Cardiol 69, 1715–1717 (2017). - PubMed
-
- Colvin M et al. OPTN/SRTR 2017 Annual Data Report: Heart. Am J Transplant 19 Suppl 2, 323–403 (2019). - PubMed
-
- Thomas SS & D’Alessandro DA Traumatic Brains and Broken Hearts: Mending the Donor Shortage in Cardiac Transplantation. J Am Coll Cardiol 70, 1259–1261 (2017). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
