

Functional Precision Medicine Provides Clinical Benefit in Advanced Aggressive Hematologic Cancers and Identifies Exceptional Responders
- PMID: 34635570
- PMCID: PMC9762339
- DOI: 10.1158/2159-8290.CD-21-0538
Functional Precision Medicine Provides Clinical Benefit in Advanced Aggressive Hematologic Cancers and Identifies Exceptional Responders
Abstract
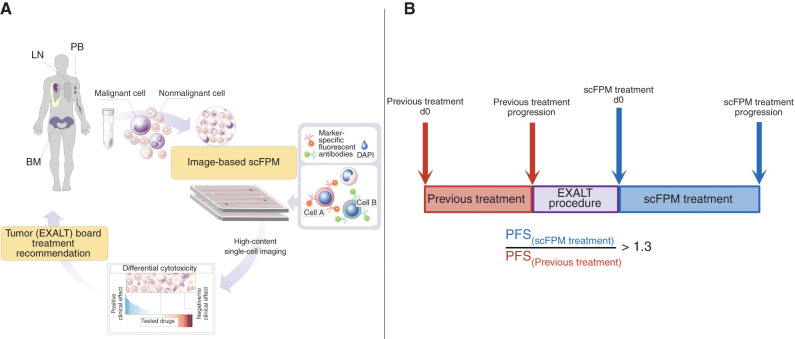
Personalized medicine aims to match the right drug with the right patient by using specific features of the individual patient's tumor. However, current strategies of personalized therapy matching provide treatment opportunities for less than 10% of patients with cancer. A promising method may be drug profiling of patient biopsy specimens with single-cell resolution to directly quantify drug effects. We prospectively tested an image-based single-cell functional precision medicine (scFPM) approach to guide treatments in 143 patients with advanced aggressive hematologic cancers. Fifty-six patients (39%) were treated according to scFPM results. At a median follow-up of 23.9 months, 30 patients (54%) demonstrated a clinical benefit of more than 1.3-fold enhanced progression-free survival compared with their previous therapy. Twelve patients (40% of responders) experienced exceptional responses lasting three times longer than expected for their respective disease. We conclude that therapy matching by scFPM is clinically feasible and effective in advanced aggressive hematologic cancers. SIGNIFICANCE: This is the first precision medicine trial using a functional assay to instruct n-of-one therapies in oncology. It illustrates that for patients lacking standard therapies, high-content assay-based scFPM can have a significant value in clinical therapy guidance based on functional dependencies of each patient's cancer.See related commentary by Letai, p. 290.This article is highlighted in the In This Issue feature, p. 275.
©2021 The Authors; Published by the American Association for Cancer Research.
Figures

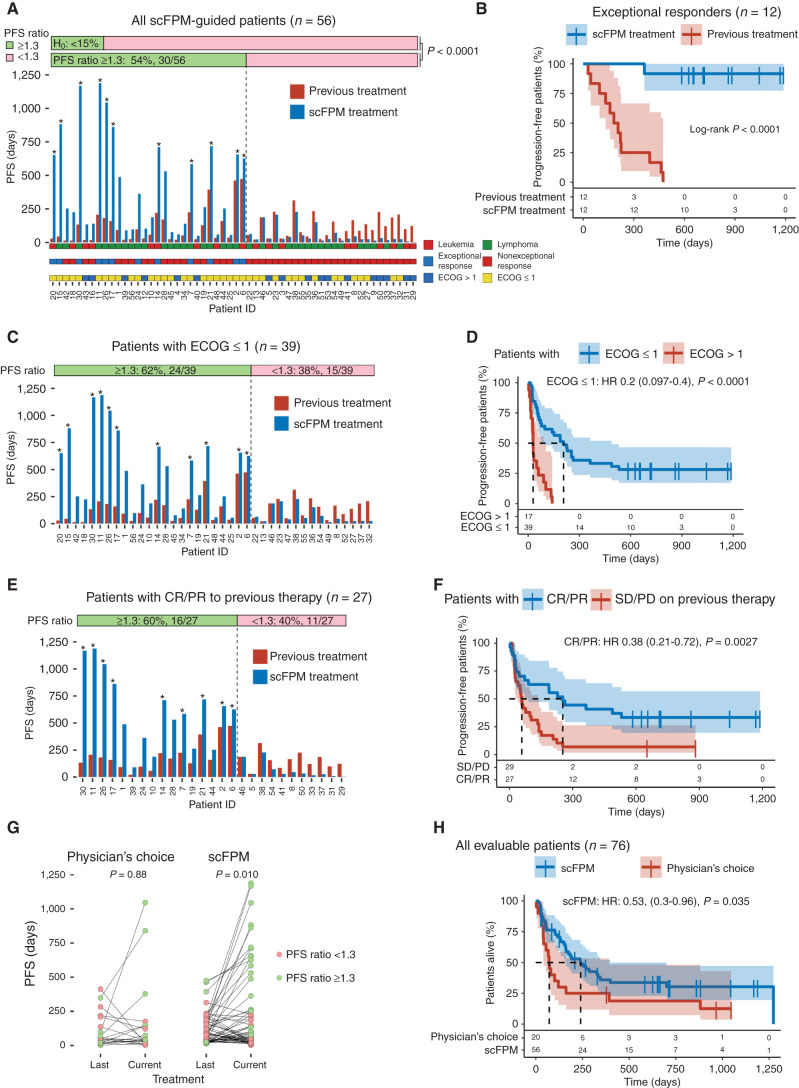
![Figure 4. Post hoc analysis. A, Kaplan–Meier plot comparing scFPM-matched treatment with previous treatment. Dotted line denotes 1-year follow-up. B, Kaplan–Meier plot comparing non–scFPM-matched treatment with previous treatment. C, Paired scatter plot comparing nonmatched versus matched patients with regard to PFS ratio. Paired Wilcoxon test comparing PFS of previous treatment versus scFPM-matched/nonmatched treatment [H0: rank PFS(previous) = rank PFS(current)]. D, Kaplan–Meier plot of scFPM-matched treatment stratified according to ECOG <1 versus ECOG ≥1. E, Kaplan–Meier plot of scFPM-matched treatment stratified according to response on previous treatment. F, Kaplan–Meier plots comparing PFS for scFPM-matched patients stratified according to tumor cell content in the sample (high ≥50%, medium >10%, low ≥10%).](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/6db0/9762339/d19942be6d75/372fig4.jpg)
Comment in
-
Functional Precision Medicine: Putting Drugs on Patient Cancer Cells and Seeing What Happens.Cancer Discov. 2022 Feb;12(2):290-292. doi: 10.1158/2159-8290.CD-21-1498. Cancer Discov. 2022. PMID: 35140175 Free PMC article.
References
-
- Tourneau CL, Delord J-P, Gonçalves A, Gavoille C, Dubot C, Isambert Net al. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): a multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncology 2015;16:1324–34. - PubMed
-
- Wheler JJ, Janku F, Naing A, Li Y, Stephen B, Zinner Ret al. Cancer therapy directed by comprehensive genomic profiling: a single center study. Cancer Res 2016;76:3690–701. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
