

Immunogenicity and Safety of a 3-Antigen Hepatitis B Vaccine vs a Single-Antigen Hepatitis B Vaccine: A Phase 3 Randomized Clinical Trial
- PMID: 34636914
- PMCID: PMC8511978
- DOI: 10.1001/jamanetworkopen.2021.28652
Immunogenicity and Safety of a 3-Antigen Hepatitis B Vaccine vs a Single-Antigen Hepatitis B Vaccine: A Phase 3 Randomized Clinical Trial
Abstract
Importance: There is a need for improved immunogenicity of hepatitis B virus (HBV) vaccines among young adults with risk of infection.
Objectives: To demonstrate manufacturing equivalence of a 3-antigen (3A) HBV vaccine, evaluate noninferiority of seroprotection rate (SPR) of 3A-HBV vs single-antigen (1A) HBV after 2 and 3 vaccine doses, and compare safety and reactogenicity between 3A-HBV and 1A-HBV vaccines.
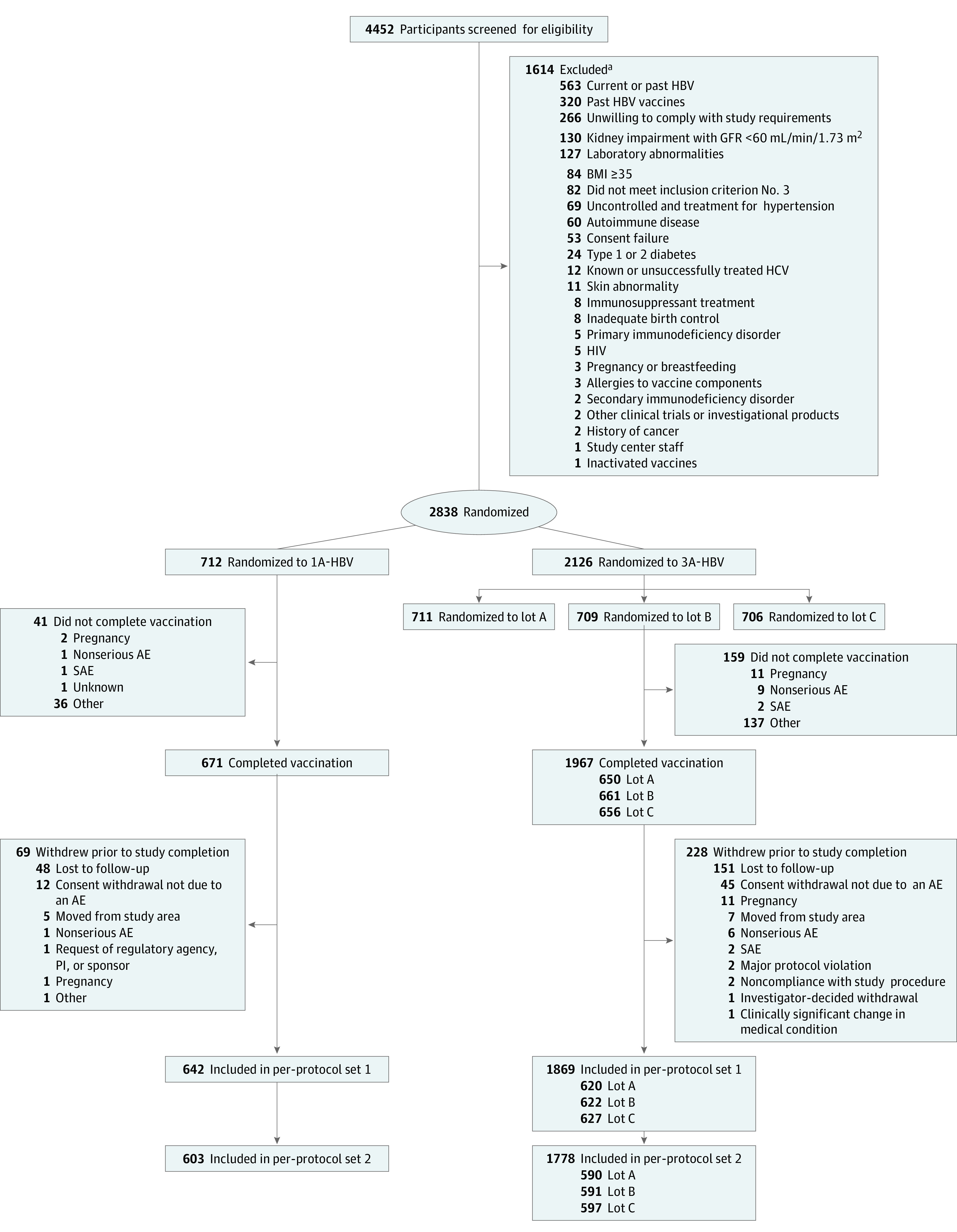
Design, setting, and participants: This phase 3, double-blinded, randomized clinical trial included healthy adults aged 18 to 45 years randomized to 1 of three 3A-HBV groups or 1 control group receiving 1A-HBV. The trial was conducted at 37 community clinics and academic hospitals in Canada, Europe, the United Kingdom, and the United States between December 2017 and October 2019. Participants were followed up for 48 weeks after the first vaccination.
Interventions: Intramuscular administration of 3A-HBV (10 μg) or 1A-HBV (20 μg) on days 0, 28, and 168.
Main outcomes and measures: Geometric mean concentration (GMC) of serum hepatitis B surface antibodies (anti-HBs) and proportion of participants achieving seroprotection.
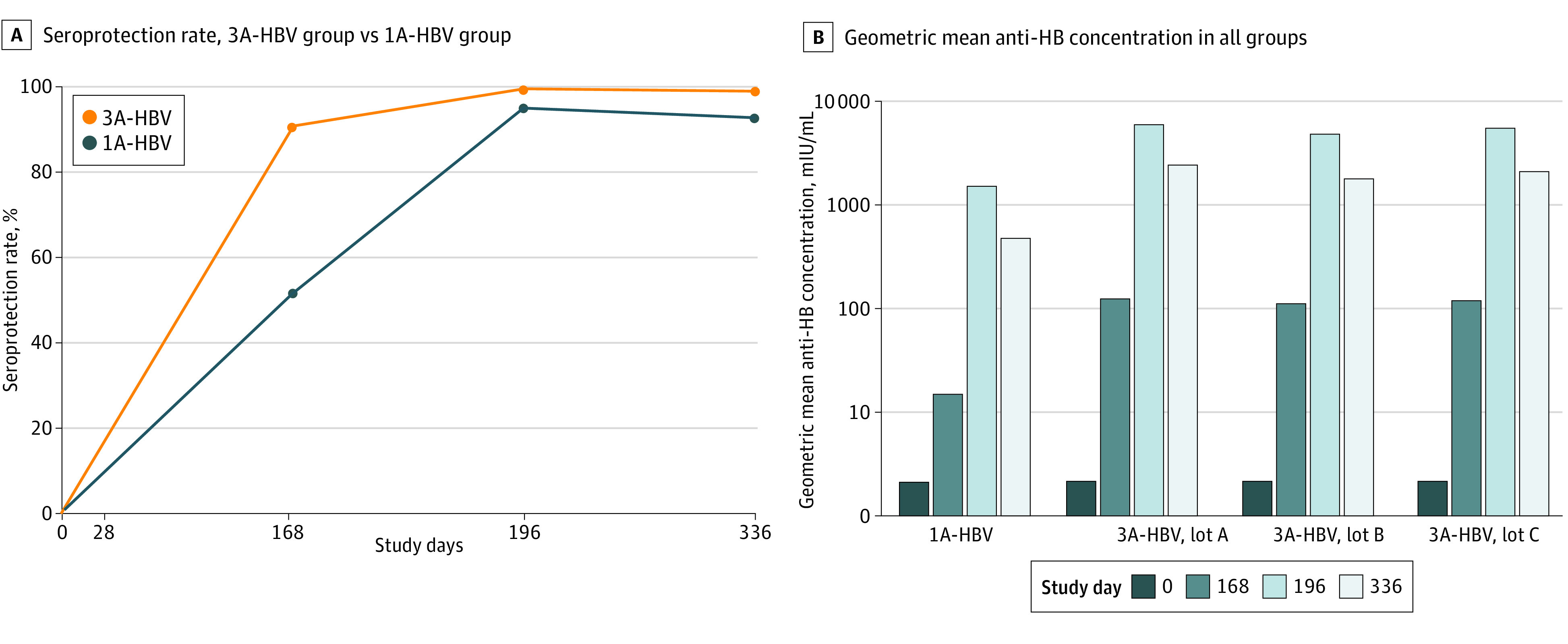
Results: Of 2838 participants, 1638 (57.8%) were women, 2595 (91.5%) were White, and 161 (5.7%) were Black or African American. A total of 712 participants (25.1%) were randomized to the 1A-HBV group and 2126 (74.9%) to 3A-HBV. The mean (SD) age at informed consent was 33.5 (8.0) years. The study demonstrated 3A-HBV lot-to-lot consistency, as the 2-sided 95% CIs for each pairwise comparison for the anti-HBs GMC ratios were within 0.67 and 1.50 (eg, adjusted GMC ratio, lot A vs lot B: 0.82; 95% CI, 0.67-1.00; lot A vs lot C: 0.95; 95% CI, 0.78-1.15; lot B vs lot C: 1.16; 95% CI, 0.95-1.41). The SPR of the pooled 3A-HBV was noninferior to 1A-HBV and higher than 1A-HBV after 2 vaccinations at day 168 (90.4% [95% CI, 89.0%-91.8%] vs 51.6% [95% CI, 47.5%-55.6%]) and 3 vaccinations at day 196 (99.3% [95% CI, 98.7%-99.6%] vs 94.8% [95% CI, 92.7%-96.4%]). The mean GMC of anti-HBs with 3A-HBV was 7.9 times higher after 2 vaccinations at day 168 and 3.5 times higher after 3 vaccinations at day 196 compared with 1A-HBV (after 2 vaccinations, 3A-HBV: GMC, 118.7 mIU/mL; 95% CI, 108.0-129.0 mIU/mL; SE, 1.0 mIU/mL; 1A-HBV: GMC, 15.0 mIU/mL; 95% CI, 12.9-17.5 mIU/mL; SE, 1.0 mIU/mL; after 3 vaccinations, 3A-HBV: GMC, 5442.4 mIU/mL; 95% CI, 4967.0-5963.0 mIU/mL; SE, 1.0 mIU/mL; 1A-HBV: 1567.2 mIU/mL; 95% CI, 1338.0-1834.0 mIU/mL; SE, 1.0 mIU/mL). Rates of local and systemic reactogenicities were higher with 3A-HBV compared with 1A-HBV (local: 1805 of 2124 [85.0%] vs 469 of 712 [65.9%]; systemic: 1445 [68.0%] vs 428 [60.1%]). Vaccine discontinuation due to adverse events (AE) was uncommon, and serious AEs were infrequent, reported in 42 participants (2.0%) and 3 participants (0.4%) in the 3A-HBV and 1A-HBV groups, respectively.
Conclusions and relevance: In this study, consistently higher antibody concentrations and SPRs were found with 3A-HBV after 2 and 3 doses vs 1A-HBV in adults aged 18 to 45 years old. The safety and efficacy of 3A-HBV shows its usefulness for the prevention of hepatitis B in young healthy adults.
Trial registration: Clinicaltrials.gov Identifier: NCT03408730; EU Clinical Trials Number: 2017-001820-22.
Conflict of interest statement
Figures
References
-
- US Department of Health and Human Services. Hepatitis B basic information. Reviewed August 31, 2021. Accessed April 3, 2020. https://www.hhs.gov/hepatitis/learn-about-viral-hepatitis/hepatitis-b-ba...
-
- US Centers for Disease Control and Prevention. Viral hepatitis surveillance: United States, 2016. Accessed April 5, 2020. https://cdc.gov/hepatitis/statistics/2016surveillance/pdfs/2016HepSurvei...
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
