

Impact on antimicrobial consumption of procalcitonin-guided antibiotic therapy for pneumonia/pneumonitis associated with aspiration in comatose mechanically ventilated patients: a multicenter, randomized controlled study
- PMID: 34636974
- PMCID: PMC8505789
- DOI: 10.1186/s13613-021-00931-4
Impact on antimicrobial consumption of procalcitonin-guided antibiotic therapy for pneumonia/pneumonitis associated with aspiration in comatose mechanically ventilated patients: a multicenter, randomized controlled study
Abstract
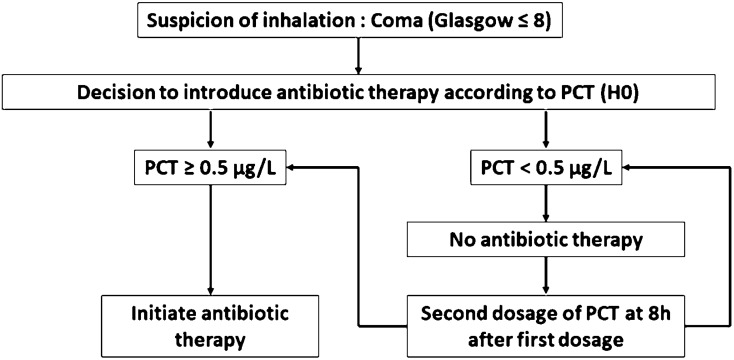
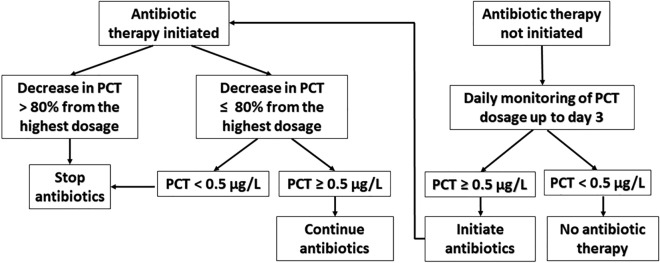
Background: In comatose patients receiving oro-tracheal intubation for mechanical ventilation (MV), the risk of aspiration is increased. Aspiration can lead to chemical pneumonitis (inflammatory reaction to the gastric contents), or aspiration pneumonia (infection caused by inhalation of microorganisms). Distinguishing between the two types is challenging. We tested the interest of using a decisional algorithm based on procalcitonin (PCT) values to guide initiation and discontinuation of antibiotic therapies in intubated patients.
Methods: The PROPASPI (PROcalcitonin Pneumonia/pneumonitis Associated with ASPIration) trial is a multicenter, prospective, randomized, controlled, single-blind, superiority study comparing two strategies: (1) an intervention group where threshold PCT values were used to guide initiation and discontinuation of antibiotics (PCT group); and (2) a control group, where antibiotic therapy was managed at the physician's discretion. Patients aged 18 years or over, intubated for coma (Glasgow score ≤ 8), with MV initiated within 48 h after admission, were eligible. The primary endpoint was the duration of antibiotic treatment during the first 15 days after admission to the ICU.
Results: From 24/2/2015 to 28/8/2019, 1712 patients were intubated for coma in the 5 participating centers, of whom 166 were included in the study. Data from 159 were available for intention-to-treat analysis: 81 in the PCT group, and 78 in the control group. Overall, 67 patients (43%) received antibiotics in the intensive care unit (ICU); there was no significant difference between groups (37 (46%) vs 30 (40%) for PCT vs control, p = 0.432). The mean duration of antibiotic treatment during the first 15 days in the ICU was 2.7 ± 3.8 days; there was no significant difference between groups (3.0 ± 4.1 days vs 2.3 ± 3.4 days for PCT vs control, p = 0.311). The mean number of days under MV was significantly higher in the PCT group (3.7 ± 3.6 days) than in controls (2.7 ± 2.5 days, p = 0.033). The duration of ICU stay was also significantly longer in the PCT group: 6.4 ± 6.5 days vs 4.6 ± 3.5 days in the control group (p = 0.043). After adjustment for SAPS II score, the difference in length of stay and duration of mechanical ventilation between groups was no longer significant.
Conclusion: The use of PCT values to guide therapy, in comparison to the use of clinical, biological (apart from PCT) and radiological criteria, does not modify exposure to antibiotics in patients intubated for coma. Trial registration Clinicaltrials.gov Identifier NCT02862314.
Keywords: Aspiration; Coma; Intensive care unit; Pneumonia; Procalcitonin.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
