

Compositional evaluation of lesion and parent bone in patients with juvenile osteochondritis dissecans of the knee using T2 * mapping
- PMID: 34637164
- PMCID: PMC9001743
- DOI: 10.1002/jor.25187
Compositional evaluation of lesion and parent bone in patients with juvenile osteochondritis dissecans of the knee using T2 * mapping
Abstract
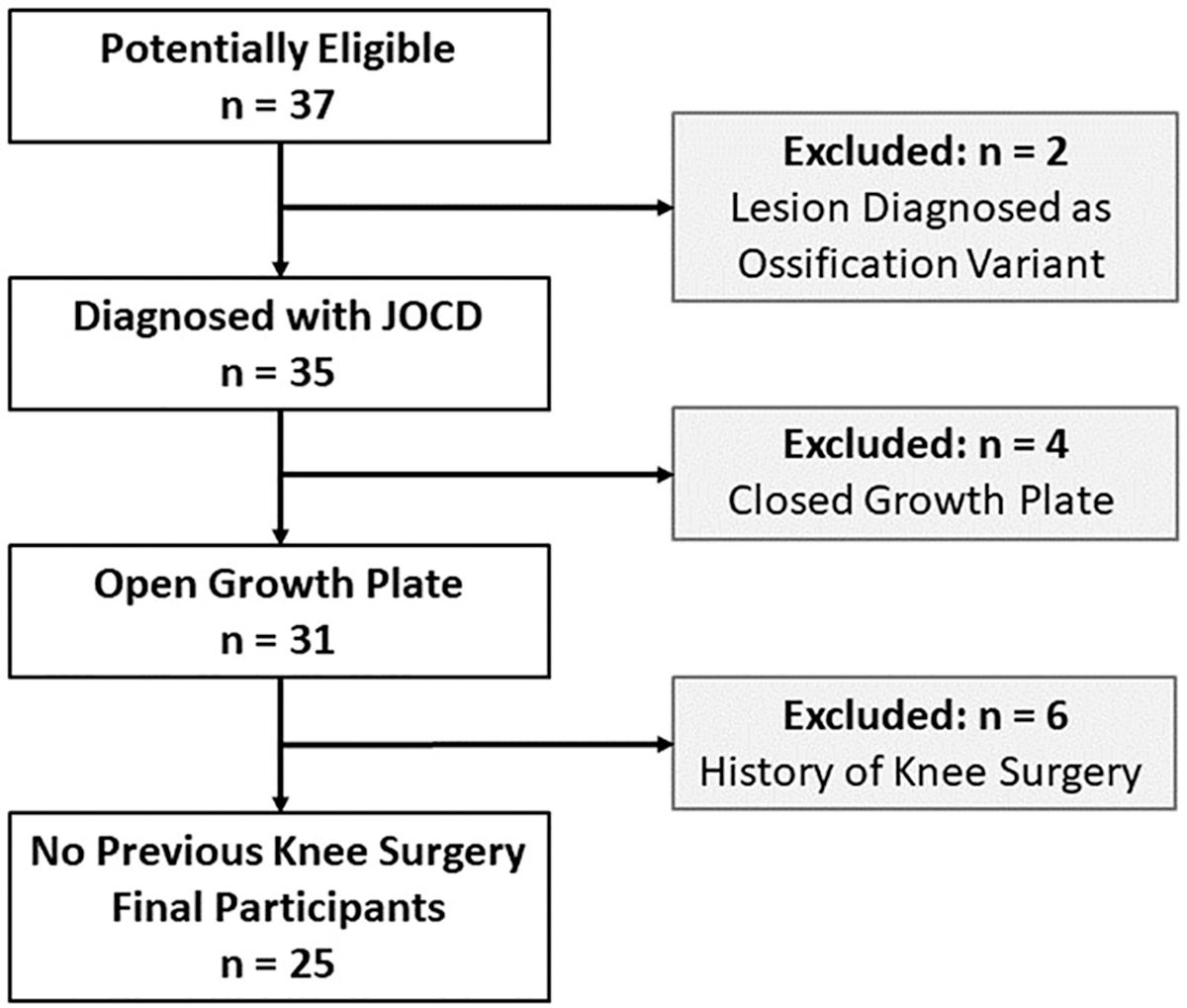
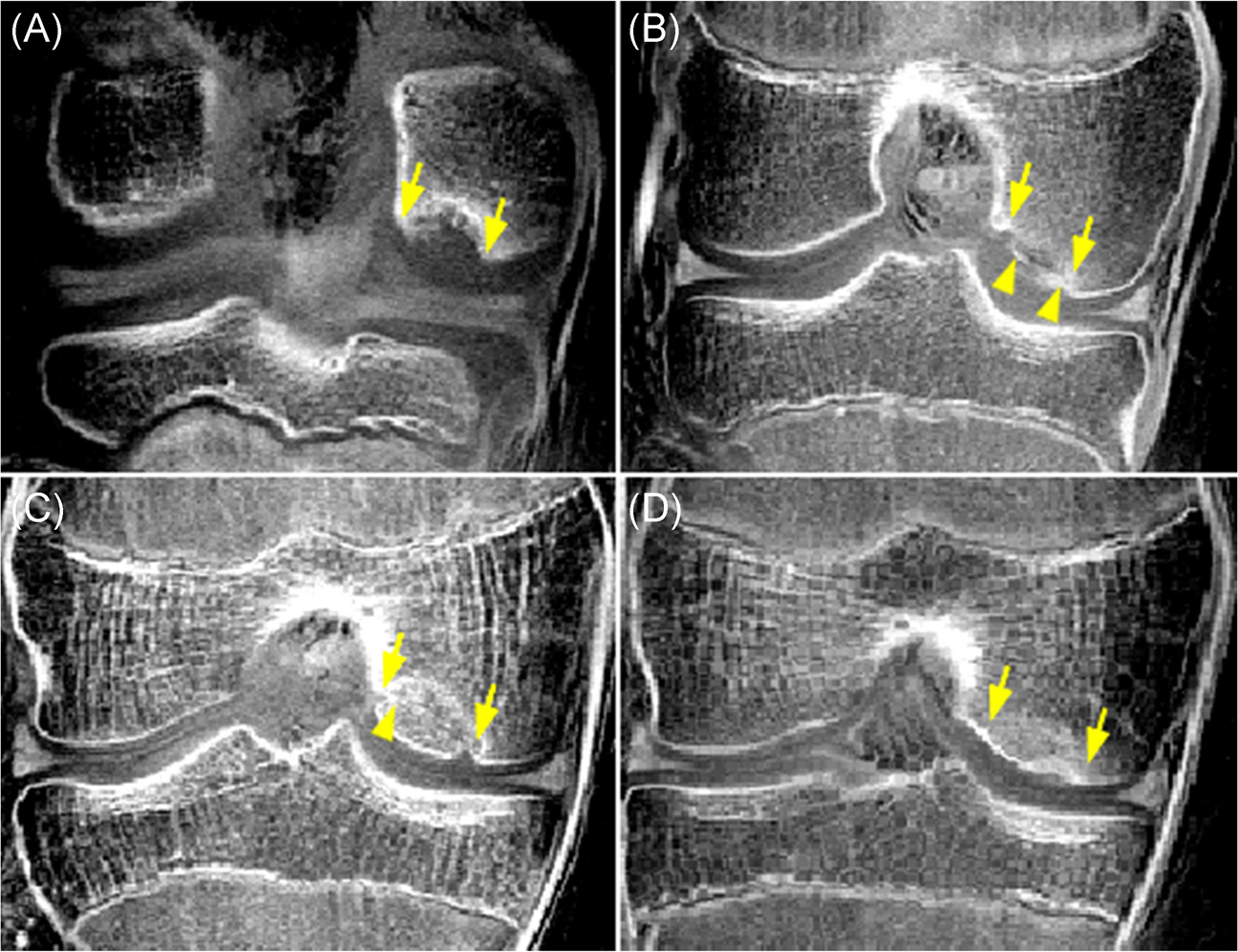
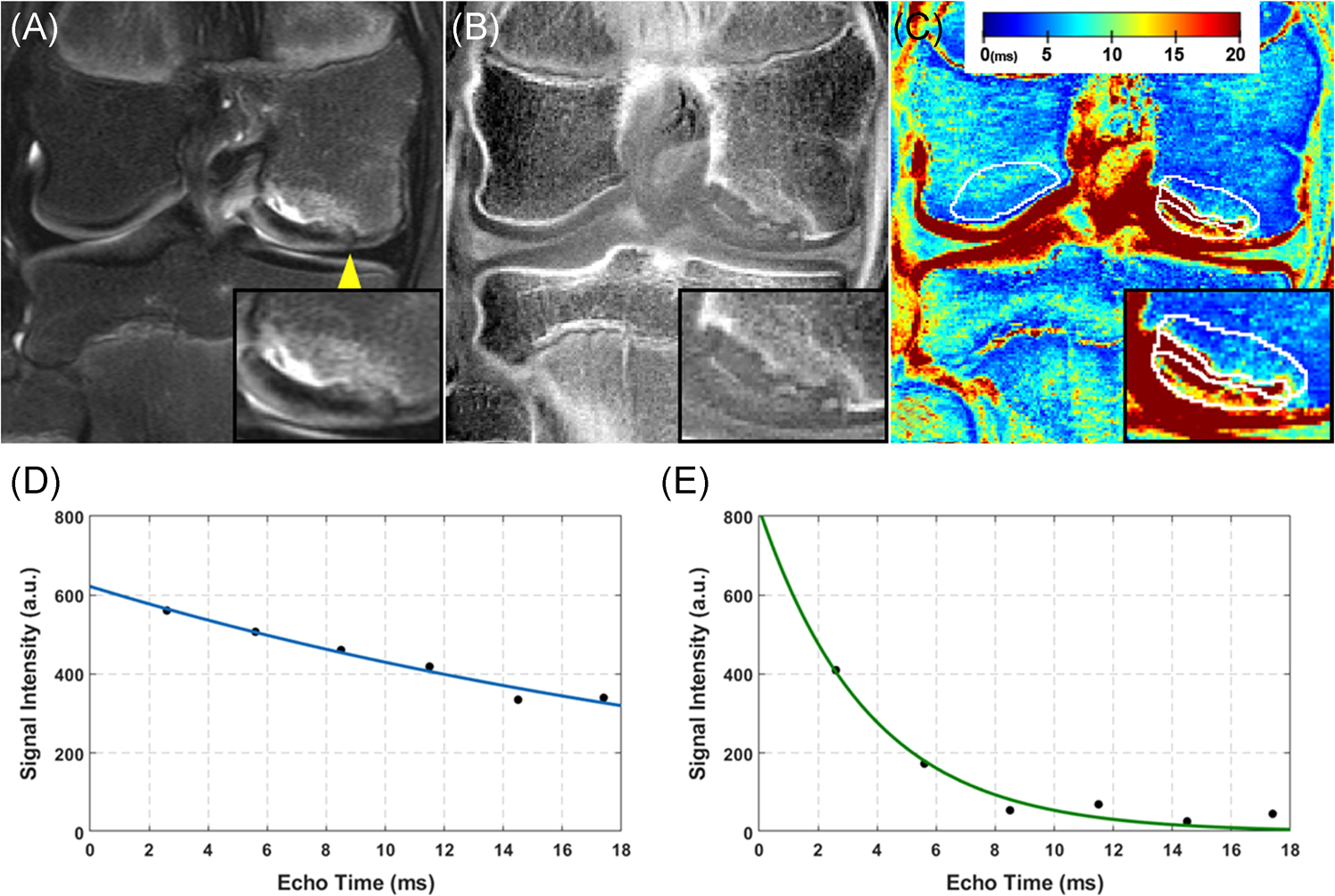
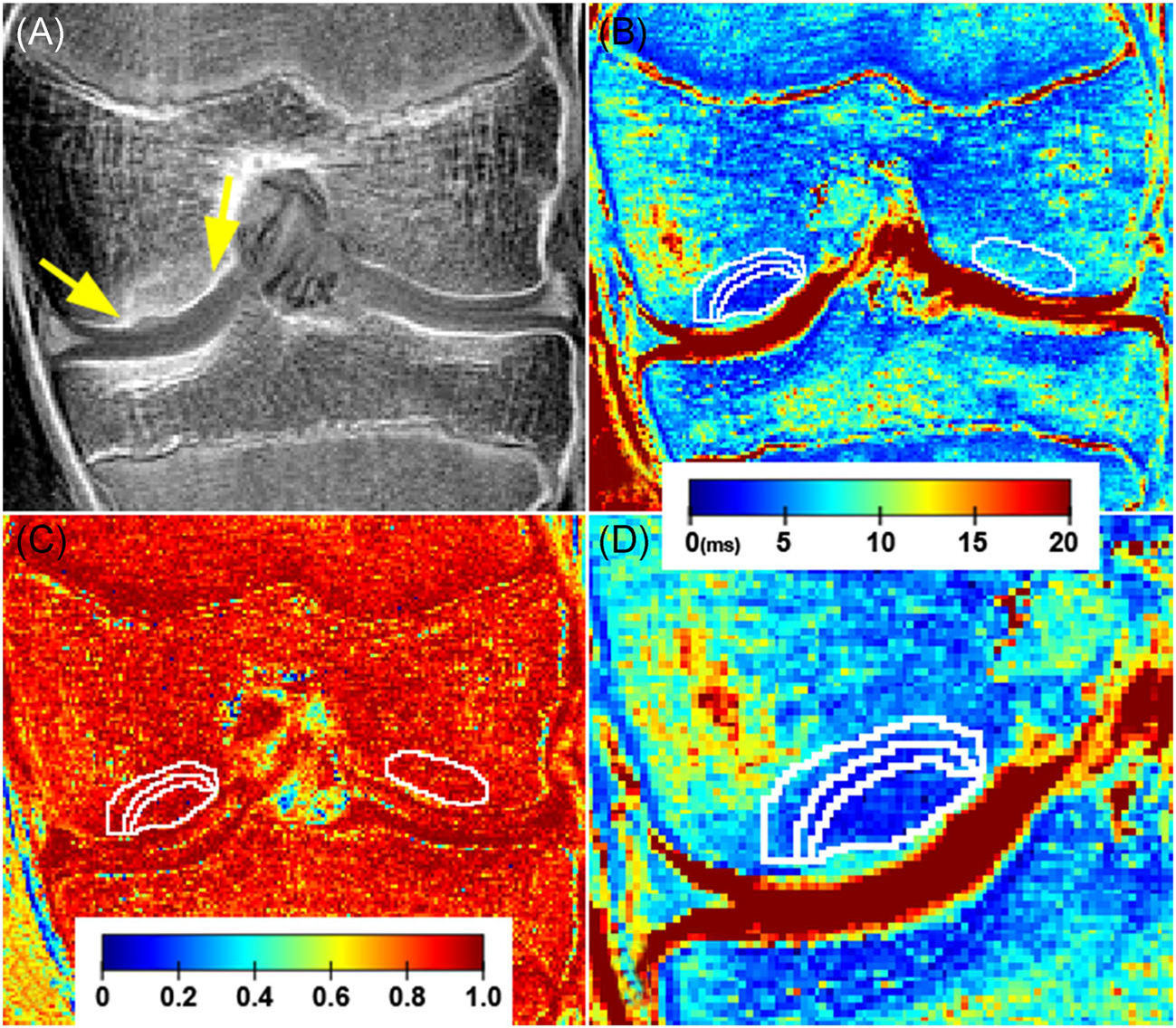
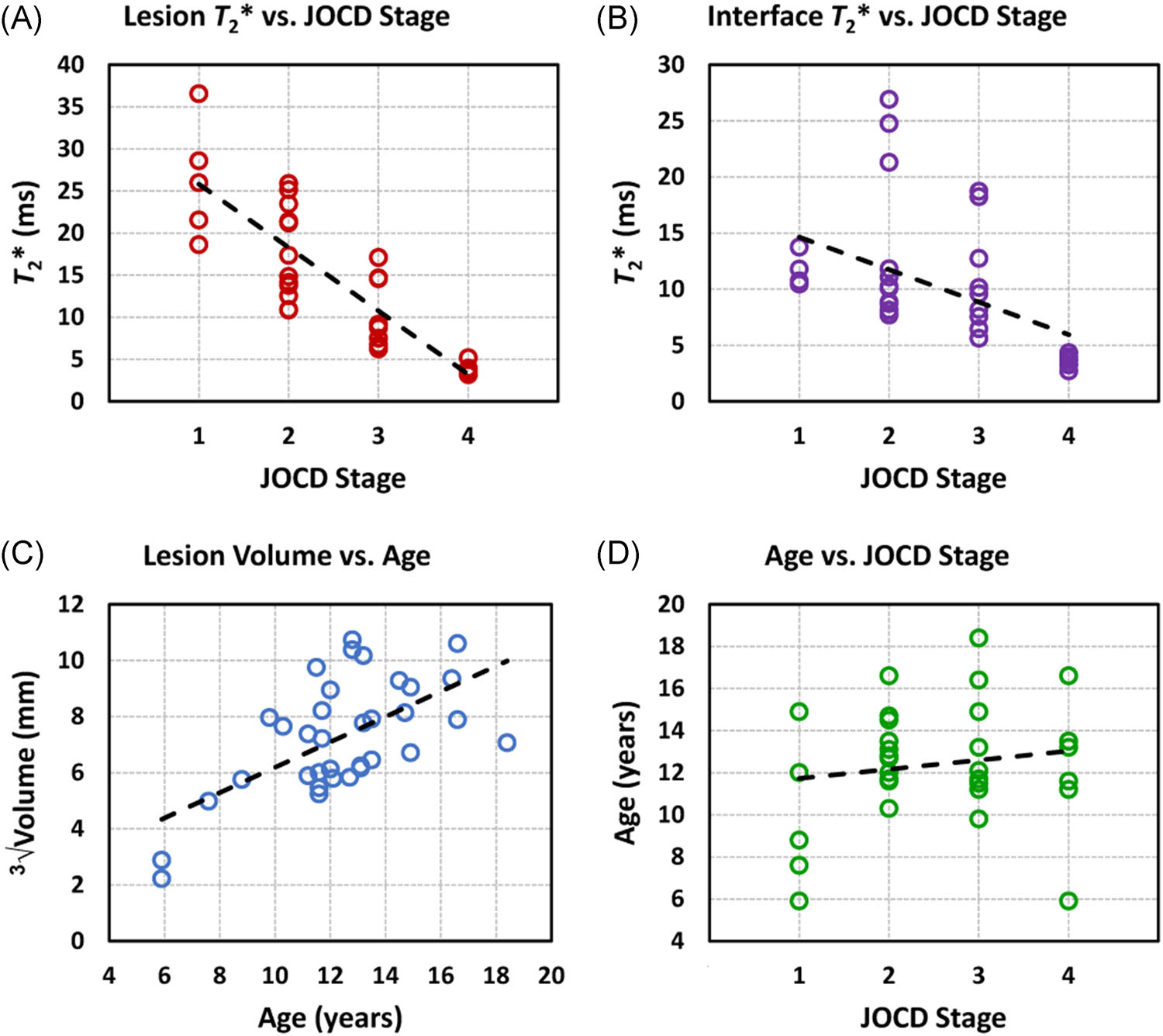
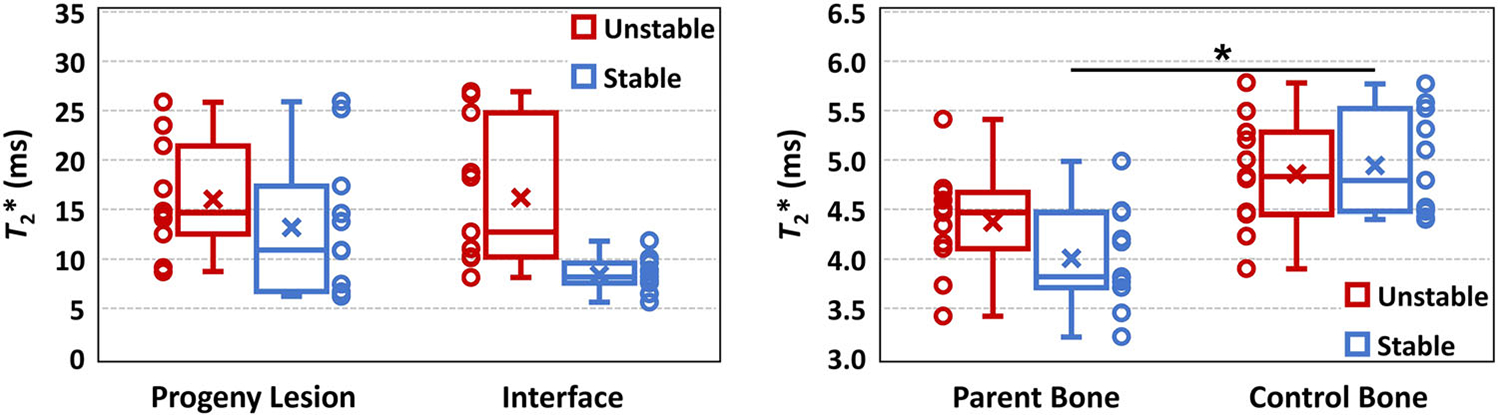
Juvenile osteochondritis dissecans (JOCD) lesions contain cartilaginous, fibrous and osseous tissues which are difficult to distinguish with clinical, morphological magnetic resonance imaging (MRI). Quantitative T2 * mapping has earlier been used to evaluate microstructure and composition of all aforementioned tissues as well as bone mineral density. However, the ability of T2 * mapping to detect changes in tissue composition between different JOCD lesion regions, different disease stages, and between stable and unstable lesions has not been demonstrated. This study analyzed morphological and T2 * MRI data from 25 patients (median age, 12.1 years) with 34 JOCD-affected and 13 healthy knees. Each lesion was assigned a stage reflecting the natural history of JOCD, with stages I and IV representing early and healed lesion, respectively. T2 * values were evaluated within the progeny lesion, interface and parent bone of each lesion and in the control bone region. T2 * was negatively correlated with JOCD stage in progeny lesion (ρ = -0.871; p < 0.001) and interface regions (ρ = -0.649; p < 0.001). Stage IV progeny showed significantly lower T2 * than control bone (p = 0.028). T2 * was significantly lower in parent bone than in control bone of patients with stable lesions (p = 0.009), but not in patients with unstable lesions (p = 0.14). Clinical significance: T2 * mapping enables differentiation between different stages of JOCD and quantitative measurement of the ossification degree in progeny lesion and interface. The observed T2 * decrease in healed and stable lesions may indicate increased bone density as a result of the active repair process. T2 * mapping provides quantitative information about JOCD lesion composition.
Keywords: T2*; compositional magnetic resonance imaging; juvenile osteochondritis dissecans; knee joint; trabecular bone.
© 2021 Orthopaedic Research Society. Published by Wiley Periodicals LLC.
Figures

References
-
- Laor T, Zbojniewicz AM, Eismann EA, Wall EJ. Juvenile osteochondritis dissecans: is it a growth disturbance of the secondary physis of the epiphysis? AJR Am J Roentgenol. 2012;199:1121–1128. - PubMed
-
- Ellermann J, Johnson CP, Wang L, Macalena JA, Nelson BJ, LaPrade RF. Insights into the epiphyseal cartilage origin and subsequent osseous manifestation of juvenile osteochondritis dissecans with a modified clinical MR imaging protocol: a pilot study. Radiology. 2017;282:798–806. - PubMed
-
- Gorbachova T, Melenevsky Y, Cohen M, Cerniglia BW. Osteochondral lesions of the knee: differentiating the most common entities at MRI. Radiographics. 2018;38:1478–1495. - PubMed
-
- Kijowski R, Blankenbaker DG, Shinki K, Fine JP, Graf BK, De Smet AA. Juvenile versus adult osteochondritis dissecans of the knee: appropriate MR imaging criteria for instability. Radiology. 2008;248:571–578. - PubMed
-
- Kessler JI, Nikizad H, Shea KG, Jacobs JC Jr, Bebchuk JD, Weiss JM. The demographics and epidemiology of osteochondritis dissecans of the knee in children and adolescents. Am J Sports Med. 2014;42:320–326. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
