

Quality of dying in hospital general wards: a cross-sectional study about the end-of-life care
- PMID: 34641824
- PMCID: PMC8507336
- DOI: 10.1186/s12904-021-00862-8
Quality of dying in hospital general wards: a cross-sectional study about the end-of-life care
Abstract
Background: In the last decade, access to national palliative care programs have improved, however a large proportion of patients continued to die in hospital, particularly within internal medicine wards.
Objectives: To describe treatments, symptoms and clinical management of adult patients at the end of their life and explore whether these differ according to expectation of death.
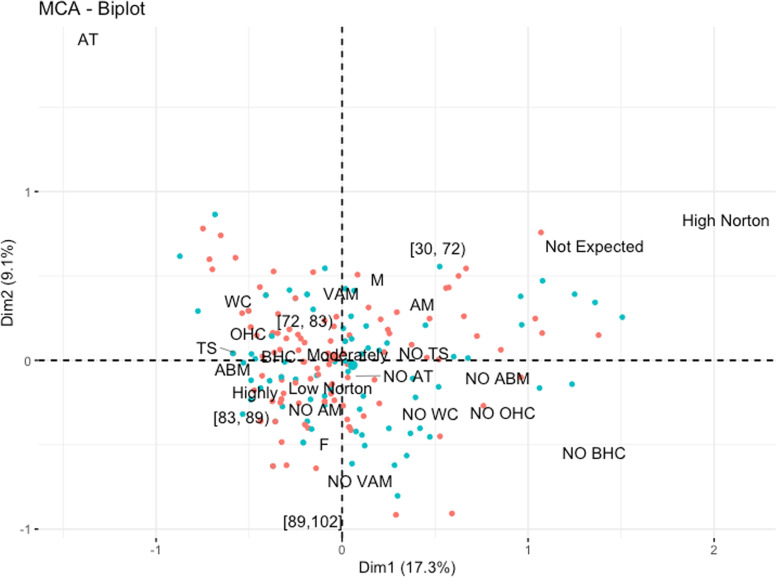
Methods: Single-centre cross-sectional study performed in the medical and surgical wards of a large tertiary-level university teaching hospital in the north of Italy. Data on nursing interventions and diagnostic procedure in proximity of death were collected after interviewing the nurse and the physician responsible for the patient. Relationship between nursing treatments delivered and patients' characteristics, quality of dying and nurses' expectation about death was summarized by means of multiple correspondence analysis (MCA).
Results: Few treatments were found statistically associated with expectation of death in the 187 patients included. In the last 48 h, routine (70.6%) and biomarkers (41.7%) blood tests were performed, at higher extent on patients whose death was not expected. Many symptoms classified as severe were reported when death was highly expected, except for agitation and respiratory fatigue which were reported when death was moderately expected. A high Norton score and absence of anti-bedsore mattress were associated with unexpected death and poor quality of dying, as summarized by MCA. Quality of dying was perceived as good by nurses when death was moderately and highly expected. Physicians rated more frequently than nurses the quality of dying as good or very good, respectively 78.6 and 57.8%, denoting a fair agreement between the two professionals (k = 0.24, P < 0.001). The palliative care consultant was requested for only two patients.
Conclusion: Staff in medical and surgical wards still deal inadequately with the needs of dying people. Presence of hospital-based specialist palliative care could lead to improvements in the patients' quality of life.
Keywords: End-of-life; Hospital death; Palliative care; Quality of death; Symptom control.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Pivodic L, Pardon K, Morin L, Addington-Hall J, Miccinesi G, Cardenas-Turanzas M, et al. Place of death in the population dying from diseases indicative of palliative care need: a cross-national population-level study in 14 countries. J Epidemiol Community Health. 2016;70:17–24. doi: 10.1136/jech-2014-205365. - DOI - PubMed
-
- Casale G, Calvieri A. Le cure palliative in Italia: inquadramento storico palliative care in Italy: a historical perspective. Medic- Metodol Didatt e Innov Clin. 2014;22:21–26.
-
- Masella C, Garavaglia G, Borghi G, Castelli A, Radaelli G, Peruselli C. Implementation of a hospital-based home palliative care at regional level: a quantitative study of the ospedalizzazione domiciliare cure palliative oncologiche program in Lombardy. Palliat Med. 2015;29:241–248. doi: 10.1177/0269216314558156. - DOI - PubMed
-
- Lusiani L, Bordin G, Mantineo G, Roncato P, Favaro L, Tessaro L, et al. Cure di fine vita nei pazienti oncologici terminali in Medicina Interna. Ital J Med. 2012;6:110–115. doi: 10.1016/j.itjm.2011.08.004. - DOI
