

Development and validation of a novel online calculator for estimating survival benefit of adjuvant transcatheter arterial chemoembolization in patients undergoing surgery for hepatocellular carcinoma
- PMID: 34641921
- PMCID: PMC8507320
- DOI: 10.1186/s13045-021-01180-5
Development and validation of a novel online calculator for estimating survival benefit of adjuvant transcatheter arterial chemoembolization in patients undergoing surgery for hepatocellular carcinoma
Abstract
Background and aims: Although adjuvant transcatheter arterial chemoembolization (TACE) for resected hepatocellular carcinoma (HCC) may improve survival for some patients, identifying which patients can benefit remains challenging. The present study aimed to construct a survival prediction calculator for individualized estimating the net survival benefit of adjuvant TACE for patients with resected HCC.
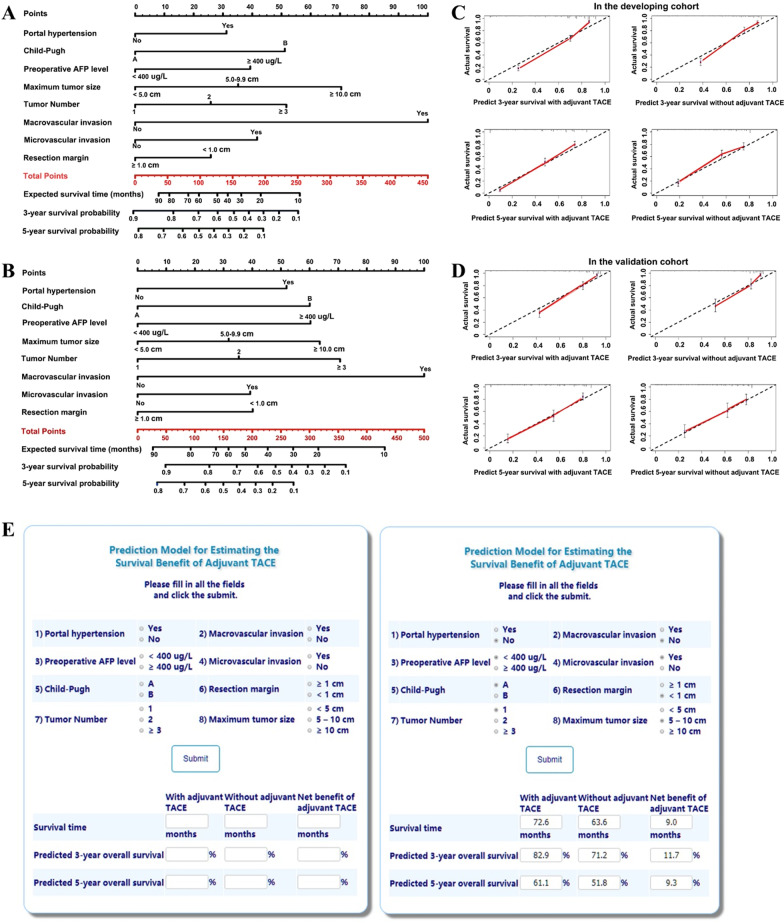
Methods: From a multicenter database, consecutive patients undergoing curative resection for HCC were enrolled and divided into the developing and validation cohorts. Using the independent survival predictors in the developing cohort, two nomogram models were constructed for patients with and without adjuvant TACE, respectively, which predictive performance was validated internally and externally by measuring concordance index (C-index) and calibration. The difference between two estimates of the prediction models was the expected survival benefit of adjuvant TACE.
Results: A total of 2514 patients met the inclusion criteria for the study. The nomogram prediction models for patients with and without adjuvant TACE were, respectively, built by incorporating the same eight independent survival predictors, including portal hypertension, Child-Pugh score, alpha-fetoprotein level, tumor size and number, macrovascular and microvascular invasion, and resection margin. These two prediction models demonstrated good calibration and discrimination, with all the C-indexes of greater than 0.75 in the developing and validation cohorts. A browser-based calculator was generated for individualized estimating the net survival benefit of adjuvant TACE.
Conclusions: Based on large-scale real-world data, an easy-to-use online calculator can be adopted as a decision aid to predict which patients with resected HCC can benefit from adjuvant TACE.
Keywords: Adjuvant therapy; Hepatectomy; Hepatocellular carcinoma; Survival; Transcatheter arterial chemoembolization.
© 2021. The Author(s).
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures
Similar articles
-
Prognostic nomogram for patients with hepatocellular carcinoma underwent adjuvant transarterial chemoembolization following curative resection.Medicine (Baltimore). 2017 Mar;96(11):e6140. doi: 10.1097/MD.0000000000006140. Medicine (Baltimore). 2017. PMID: 28296727 Free PMC article.
-
Prognostic nomogram for post-surgical treatment with adjuvant TACE in hepatitis B virus-related hepatocellular carcinoma.Oncotarget. 2016 Sep 6;7(36):58302-58314. doi: 10.18632/oncotarget.11078. Oncotarget. 2016. PMID: 27506942 Free PMC article.
-
Clinical efficacy of postoperative adjuvant transcatheter arterial chemoembolization on hepatocellular carcinoma.World J Surg Oncol. 2016 Apr 2;14:100. doi: 10.1186/s12957-016-0855-z. World J Surg Oncol. 2016. PMID: 27038790 Free PMC article.
-
Resection Plus Post-operative Adjuvant Transcatheter Arterial Chemoembolization (TACE) Compared with Resection Alone for Hepatocellular Carcinoma: A Systematic Review and Meta-analysis.Cardiovasc Intervent Radiol. 2020 Apr;43(4):572-586. doi: 10.1007/s00270-019-02392-6. Epub 2020 Jan 2. Cardiovasc Intervent Radiol. 2020. PMID: 31897617
-
Adjuvant transarterial chemoembolization after curative hepatectomy for hepatocellular carcinoma with microvascular invasion: A systematic review and meta-analysis.Clin Res Hepatol Gastroenterol. 2020 Apr;44(2):142-154. doi: 10.1016/j.clinre.2019.06.012. Epub 2019 Jul 11. Clin Res Hepatol Gastroenterol. 2020. PMID: 31303533
Cited by
-
Adjuvant and Neoadjuvant Treatments for Resectable Hepatocellular Carcinoma.Curr Oncol Rep. 2023 Oct;25(10):1191-1201. doi: 10.1007/s11912-023-01455-9. Epub 2023 Sep 9. Curr Oncol Rep. 2023. PMID: 37688739 Free PMC article. Review.
-
Impact of Hepatic Pedicle Clamping on Long-Term Survival Following Hepatectomy for Hepatocellular Carcinoma: Stratified Analysis Based on Intraoperative Blood Transfusion Status.Ann Surg Oncol. 2024 Mar;31(3):1812-1822. doi: 10.1245/s10434-023-14642-6. Epub 2023 Dec 1. Ann Surg Oncol. 2024. PMID: 38038790
-
Development and validation of a model for predicting who can benefit from multiple TACE in HCC patients.Clin Exp Med. 2024 Nov 2;25(1):1. doi: 10.1007/s10238-024-01516-8. Clin Exp Med. 2024. PMID: 39487889 Free PMC article.
-
Machine Learning Model Based on the Neutrophil-to-Eosinophil Ratio Predicts the Recurrence of Hepatocellular Carcinoma After Surgery.J Hepatocell Carcinoma. 2024 Apr 3;11:679-691. doi: 10.2147/JHC.S455612. eCollection 2024. J Hepatocell Carcinoma. 2024. PMID: 38585292 Free PMC article.
-
Enhanced interactions within microenvironment accelerates dismal prognosis in HBV-related HCC after TACE.Hepatol Commun. 2024 Oct 3;8(10):e0548. doi: 10.1097/HC9.0000000000000548. eCollection 2024 Oct 1. Hepatol Commun. 2024. PMID: 39365124 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
