

Multinational characterization of neurological phenotypes in patients hospitalized with COVID-19
- PMID: 34642371
- PMCID: PMC8510999
- DOI: 10.1038/s41598-021-99481-9
Multinational characterization of neurological phenotypes in patients hospitalized with COVID-19
Abstract
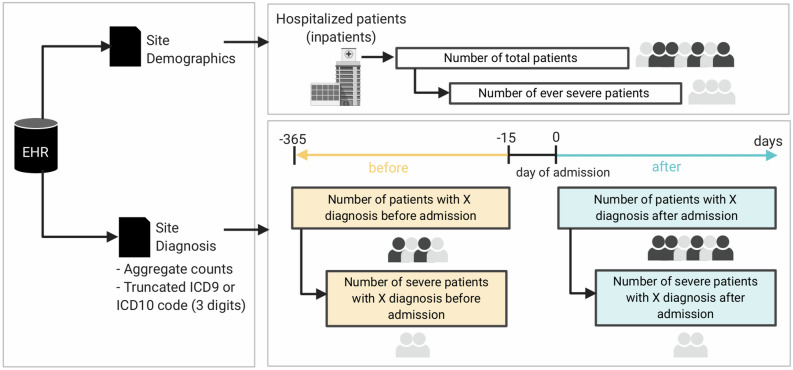
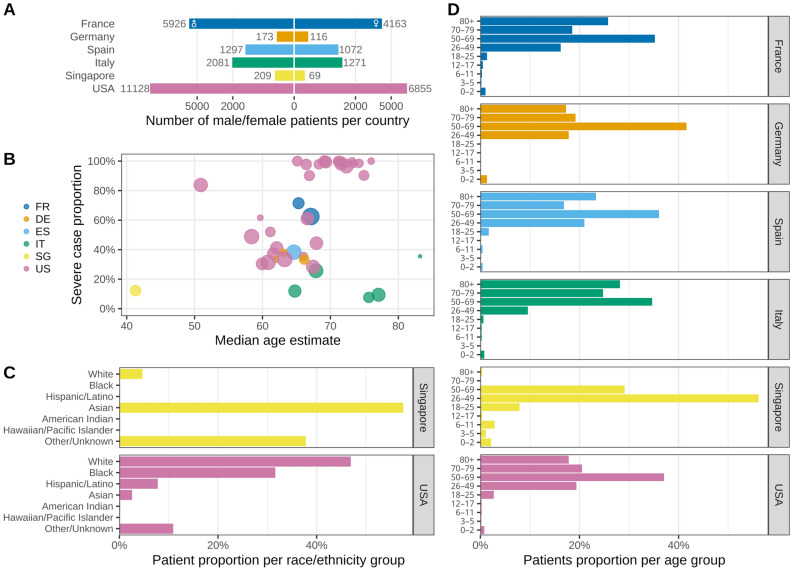
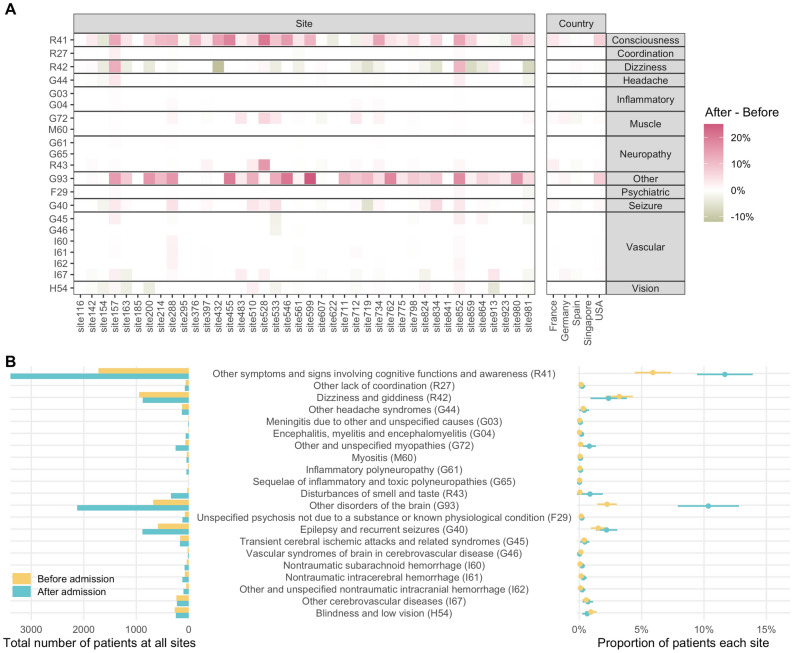
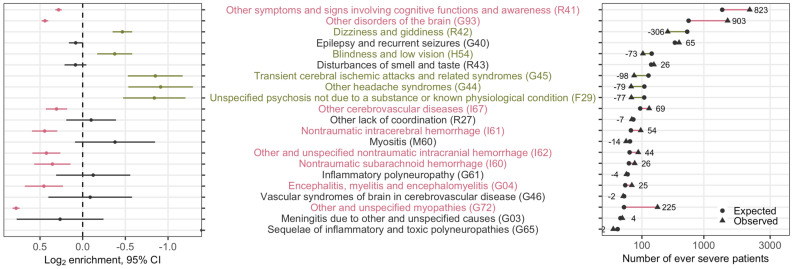
Neurological complications worsen outcomes in COVID-19. To define the prevalence of neurological conditions among hospitalized patients with a positive SARS-CoV-2 reverse transcription polymerase chain reaction test in geographically diverse multinational populations during early pandemic, we used electronic health records (EHR) from 338 participating hospitals across 6 countries and 3 continents (January-September 2020) for a cross-sectional analysis. We assessed the frequency of International Classification of Disease code of neurological conditions by countries, healthcare systems, time before and after admission for COVID-19 and COVID-19 severity. Among 35,177 hospitalized patients with SARS-CoV-2 infection, there was an increase in the proportion with disorders of consciousness (5.8%, 95% confidence interval [CI] 3.7-7.8%, pFDR < 0.001) and unspecified disorders of the brain (8.1%, 5.7-10.5%, pFDR < 0.001) when compared to the pre-admission proportion. During hospitalization, the relative risk of disorders of consciousness (22%, 19-25%), cerebrovascular diseases (24%, 13-35%), nontraumatic intracranial hemorrhage (34%, 20-50%), encephalitis and/or myelitis (37%, 17-60%) and myopathy (72%, 67-77%) were higher for patients with severe COVID-19 when compared to those who never experienced severe COVID-19. Leveraging a multinational network to capture standardized EHR data, we highlighted the increased prevalence of central and peripheral neurological phenotypes in patients hospitalized with COVID-19, particularly among those with severe disease.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Update of
-
Multinational Prevalence of Neurological Phenotypes in Patients Hospitalized with COVID-19.medRxiv [Preprint]. 2021 Jan 29:2021.01.27.21249817. doi: 10.1101/2021.01.27.21249817. medRxiv. 2021. Update in: Sci Rep. 2021 Oct 12;11(1):20238. doi: 10.1038/s41598-021-99481-9. PMID: 33655281 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Grants and funding
- R01NS098023/NS/NINDS NIH HHS/United States
- UL1 TR001857/TR/NCATS NIH HHS/United States
- UL1 TR001878/TR/NCATS NIH HHS/United States
- U24 CA210967/CA/NCI NIH HHS/United States
- R01 NS098023/NS/NINDS NIH HHS/United States
- UL1 TR001422/TR/NCATS NIH HHS/United States
- UL1 TR002366/TR/NCATS NIH HHS/United States
- P30 ES017885/ES/NIEHS NIH HHS/United States
- L40 HL148910/HL/NHLBI NIH HHS/United States
- R01 LM012095/LM/NLM NIH HHS/United States
- CTSA Award #UL1TR002366/TR/NCATS NIH HHS/United States
- T32 LM012203/LM/NLM NIH HHS/United States
- CTSA Award #UL1TR001878/TR/NCATS NIH HHS/United States
- UL1TR001857/TR/NCATS NIH HHS/United States
- K23HL148394/HL/NHLBI NIH HHS/United States
- FS/19/52/34563/BHF_/British Heart Foundation/United Kingdom
- UL1 TR001420/TR/NCATS NIH HHS/United States
- UL1TR001420/TR/NCATS NIH HHS/United States
- P30ES017885/ES/NIEHS NIH HHS/United States
- MC_PC_18034/MRC_/Medical Research Council/United Kingdom
- K23 HL148394/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
