

Anemia prevalence in women of reproductive age in low- and middle-income countries between 2000 and 2018
- PMID: 34642490
- PMCID: PMC8516651
- DOI: 10.1038/s41591-021-01498-0
Anemia prevalence in women of reproductive age in low- and middle-income countries between 2000 and 2018
Abstract
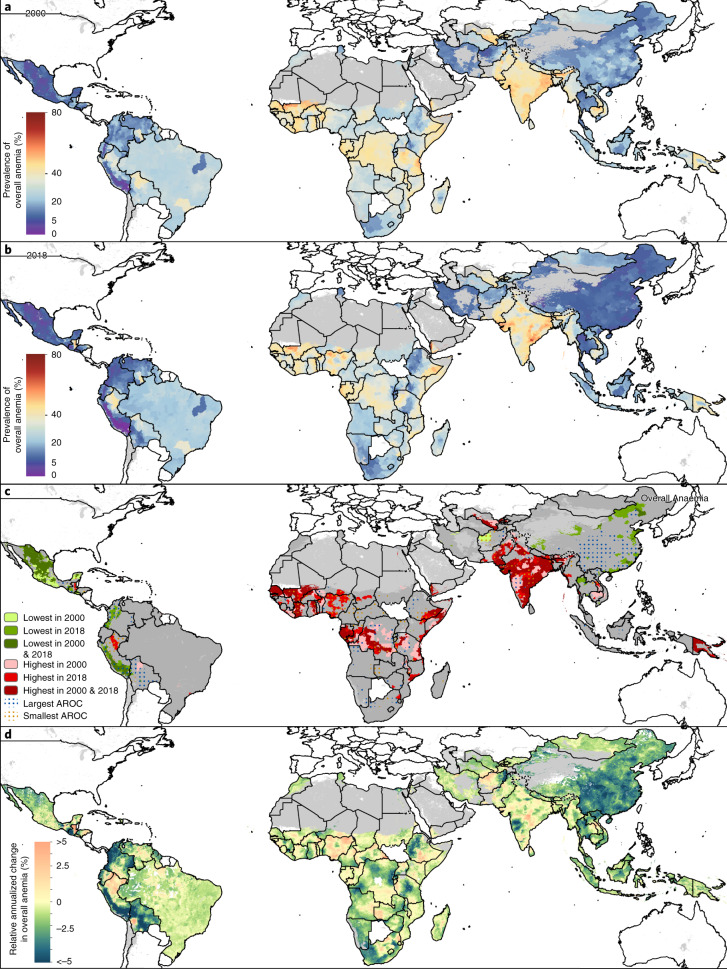
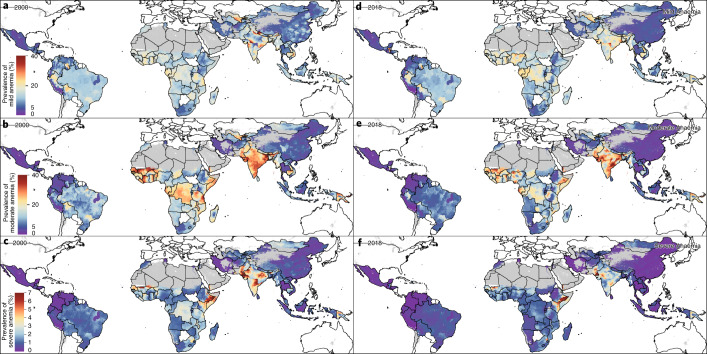
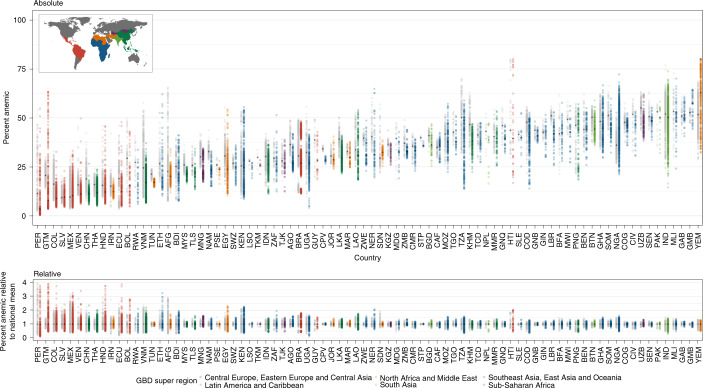
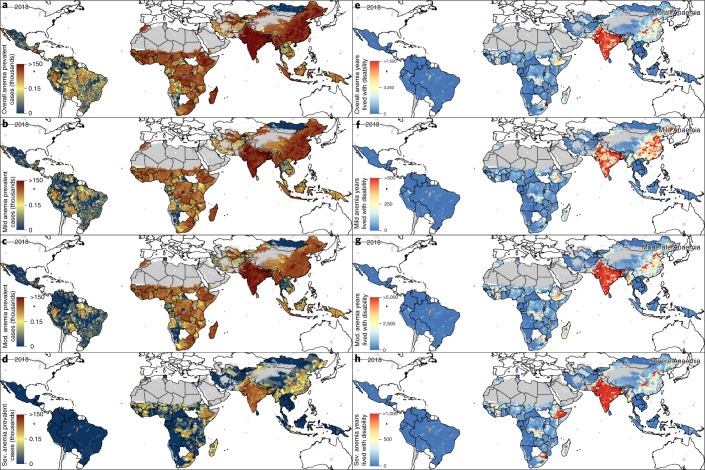
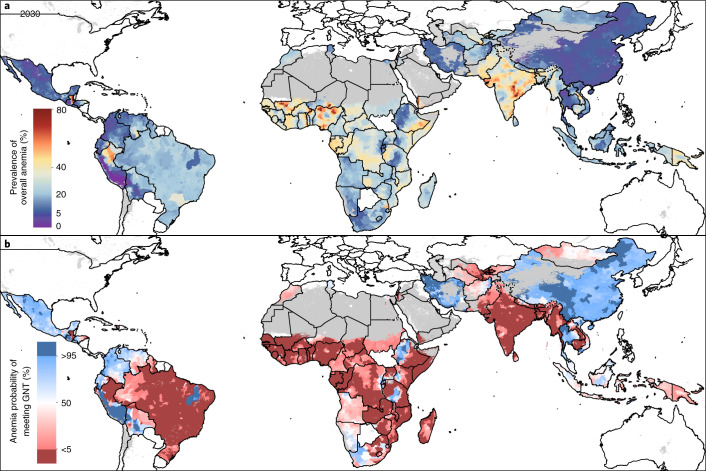
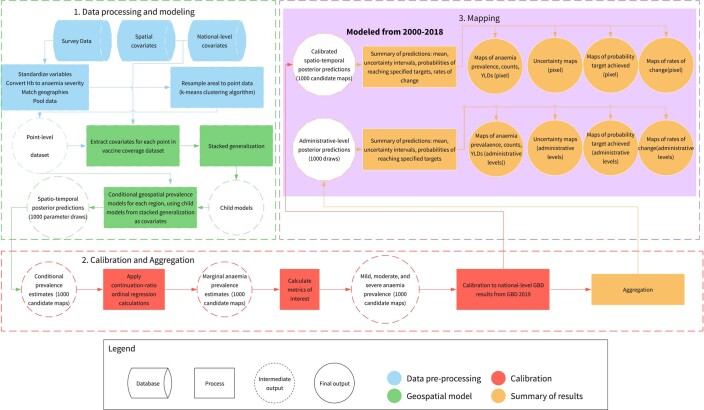
Anemia is a globally widespread condition in women and is associated with reduced economic productivity and increased mortality worldwide. Here we map annual 2000-2018 geospatial estimates of anemia prevalence in women of reproductive age (15-49 years) across 82 low- and middle-income countries (LMICs), stratify anemia by severity and aggregate results to policy-relevant administrative and national levels. Additionally, we provide subnational disparity analyses to provide a comprehensive overview of anemia prevalence inequalities within these countries and predict progress toward the World Health Organization's Global Nutrition Target (WHO GNT) to reduce anemia by half by 2030. Our results demonstrate widespread moderate improvements in overall anemia prevalence but identify only three LMICs with a high probability of achieving the WHO GNT by 2030 at a national scale, and no LMIC is expected to achieve the target in all their subnational administrative units. Our maps show where large within-country disparities occur, as well as areas likely to fall short of the WHO GNT, offering precision public health tools so that adequate resource allocation and subsequent interventions can be targeted to the most vulnerable populations.
© 2021. The Author(s).
Conflict of interest statement
This study was funded by the Bill & Melinda Gates Foundation. Co-authors employed by the Bill & Melinda Gates Foundation provided feedback on initial maps and drafts of this manuscript. Otherwise, the funders of the study had no role in study design, data collection, data analysis, data interpretation or writing of the final report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication. R.A. received consultancy/speaker fees from UCB, Sandoz, Abbvie, Zentiva, Teva, Laropharm, CEGEDIM, Angelini, Biessen Pharma, Hofigal, AstraZeneca and Stada. Dr. Bell reports grants from the Wellcome Trust Foundation, grants from the NIH, grants from the Environmental Protection Agency, personal fees from the University of Montana, other from the NIH and grants from the Yale Climate Change and Health Center, all outside of the submitted work. Dr. Gessner reports employment from Pfizer Vaccines, outside of the submitted work. Dr. Islam reports grants from the National Heart Foundation of Australia and grants from the NHMRC, outside of the submitted work. Dr. Jozwiak reports personal fees from Amgen, personal fees from Alab Laboratories, personal fees from Teva, personal fees from Synexus, personal fees from Boehringer Ingelheim and personal fees from Zentiva, outside of the submitted work. Dr. Krishan reports non-financial support from the UGC Centre of Advanced Study, CAS II, Department of Anthropology, Panjab University, outside of the submitted work. Dr. Mendoza reports employment as a program analyst in Population and Development at the United Nations Population Fund-UNFPA Country Office in Peru, which does not necessarily endorse this study. Dr. Pandi-Perumal reports non-financial support from Somnogen Canada and personal fees from royalties, outside of the submitted work. Dr. Postma reports grants and personal fees from MSD, grants and personal fees from GSK, grants and personal fees from Pfizer, grants and personal fees from Boehringer Ingelheim, grants and personal fees from Novavax, personal fees from Quintiles, grants from Bayer, grants and personal fees from BMS, grants and personal fees from Astra Zeneca, grants and personal fees from Sanofi, personal fees from Novartis, personal fees from Pharmerit, other from Health-Ecore, other from PAG, other from Asc Academics, grants and personal fees from IQVIA, grants from bioMérieux, grants from the WHO, grants from the European Union, grants and personal fees from Seqirus, grants from FIND, grants from Antilope and grants from DIKTI, LPDP, Budi, all outside of the submitted work. Dr. Rezahosseini reports grants from the Research Foundation of Rigshospitalet and grants from the A.P. Møller Fonden, outside of the submitted work. Dr. Shivarov reports salary from PRAHS, outside of the submitted work. Dr. Uddin reports as having worked as a visiting fellow at Deakin University Institute for Physical Activity and Nutrition (IPAN). IPAN paid for travel (including flights and transportation), accommodations and meals. E.Upadhyay is listed on two patents: ‘A system and method of reusable filters for anti-pollution mask’ (pending) and ‘A system and method for electricity generation through crop stubble by using microbial fuel cells’ (pending). Dr. Wu reports grants from the Ministry of Science and Technology in China, personal fees from HealthKeepers, grants from Suzhou Municipal Science and Technology Bureau and grants from Kunshan Government, outside of the submitted work. Dr. Zhu reports grants from UTHealth Innovation for Cancer Prevention Research Training Program Pre-doctoral Fellowship (Cancer Prevention and Research Institute of Texas, grant no. RP160015), during the conduct of the study.
Figures
Comment in
-
Anemia in women - an intractable problem that requires innovative solutions.Nat Med. 2021 Oct;27(10):1675-1677. doi: 10.1038/s41591-021-01514-3. Nat Med. 2021. PMID: 34642492 No abstract available.
References
-
- World Health Organization. Global nutrition targets 2025: anaemia policy brief. https://apps.who.int/iris/handle/10665/148556 (2014) .
-
- Horton S, Ross J. The economics of iron deficiency. Food Policy. 2003;28:51–75. doi: 10.1016/S0306-9192(02)00070-2. - DOI
