

The use of deep learning on endoscopic images to assess the response of rectal cancer after chemoradiation
- PMID: 34642794
- PMCID: PMC9001548
- DOI: 10.1007/s00464-021-08685-7
The use of deep learning on endoscopic images to assess the response of rectal cancer after chemoradiation
Abstract
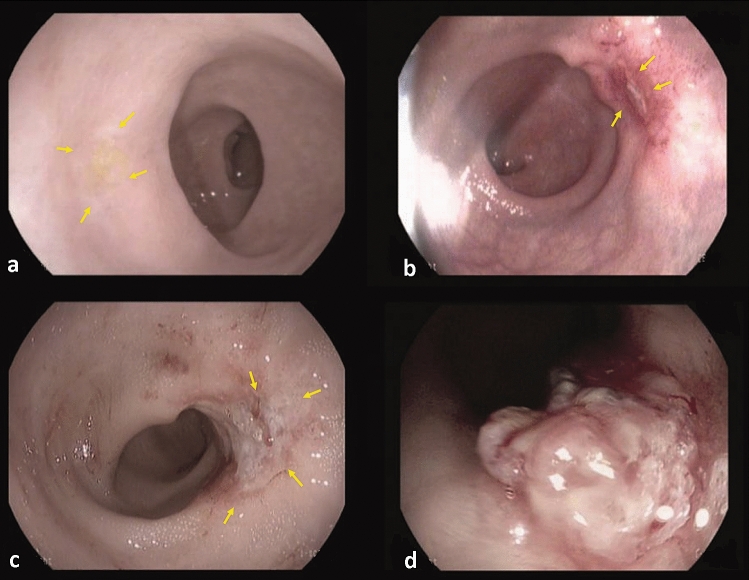
Background: Accurate response evaluation is necessary to select complete responders (CRs) for a watch-and-wait approach. Deep learning may aid in this process, but so far has never been evaluated for this purpose. The aim was to evaluate the accuracy to assess response with deep learning methods based on endoscopic images in rectal cancer patients after neoadjuvant therapy.
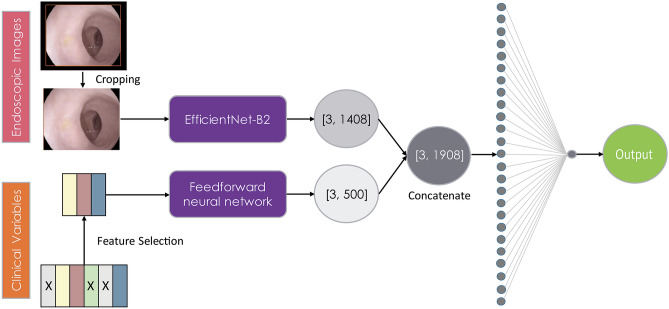
Methods: Rectal cancer patients diagnosed between January 2012 and December 2015 and treated with neoadjuvant (chemo)radiotherapy were retrospectively selected from a single institute. All patients underwent flexible endoscopy for response evaluation. Diagnostic performance (accuracy, area under the receiver operator characteristics curve (AUC), positive- and negative predictive values, sensitivities and specificities) of different open accessible deep learning networks was calculated. Reference standard was histology after surgery, or long-term outcome (>2 years of follow-up) in a watch-and-wait policy.
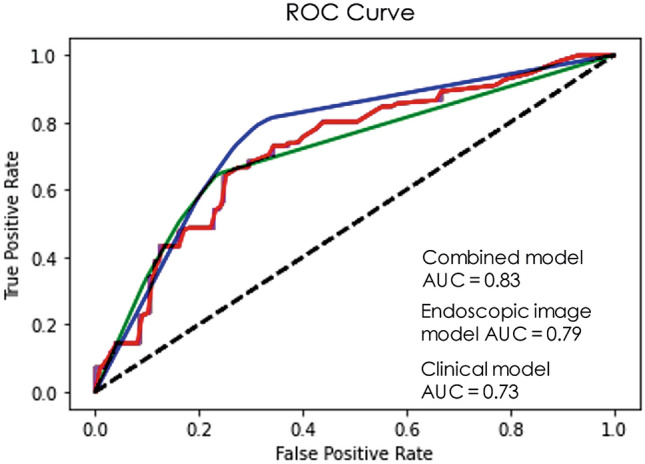
Results: 226 patients were included for the study (117(52%) were non-CRs; 109(48%) were CRs). The accuracy, AUC, positive- and negative predictive values, sensitivity and specificity of the different models varied from 0.67-0.75%, 0.76-0.83%, 67-74%, 70-78%, 68-79% to 66-75%, respectively. Overall, EfficientNet-B2 was the most successful model with the highest diagnostic performance.
Conclusions: This pilot study shows that deep learning has a modest accuracy (AUCs 0.76-0.83). This is not accurate enough for clinical decision making, and lower than what is generally reported by experienced endoscopists. Deep learning models can however be further improved and may become useful to assist endoscopists in evaluating the response. More well-designed prospective studies are required.
Keywords: Artificial intelligence; Deep learning; Organ preservation; Rectal cancer; Response evaluation; Watch-and-wait approach.
© 2021. The Author(s).
Conflict of interest statement
Hester E. Haak, Selam Waktola, Monique Maas, Sean Benson, Xinpei Gao, Regina G.H. Beets-Tan, Geerard L. Beets, Monique van Leerdam and Jarno Melenhorst have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Maas M, Lambregts DM, Nelemans PJ, Heijnen LA, Martens MH, Leijtens JW, et al. Assessment of clinical complete response after chemoradiation for rectal cancer with digital rectal examination, endoscopy, and MRI: selection for organ-saving treatment. Ann Surg Oncol. 2015;22(12):3873–3880. doi: 10.1245/s10434-015-4687-9. - DOI - PMC - PubMed
-
- van der Sande ME, Maas M, Melenhorst J, Breukink SO, van Leerdam ME, and Beets GL (2019) Predictive value of endoscopic features for a complete response after chemoradiotherapy for rectal cancer. Ann Surg. - PubMed
-
- Nahas SC, Rizkallah Nahas CS, Sparapan Marques CF, Ribeiro U, Jr, Cotti GC, Imperiale AR, et al. Pathologic complete response in rectal cancer: can we detect it? lessons learned from a proposed randomized trial of watch-and-wait treatment of rectal cancer. Dis Colon Rectum. 2016;59(4):255–263. doi: 10.1097/DCR.0000000000000558. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
