

Development and validation of a risk score to prioritize patients for evaluation of access stenosis
- PMID: 34642963
- PMCID: PMC9292738
- DOI: 10.1111/sdi.13026
Development and validation of a risk score to prioritize patients for evaluation of access stenosis
Abstract
Background: Access flow dysfunction, often associated with stenosis, is a common problem in hemodialysis access and may result in progression to thrombosis. Timely identification of accesses in need of evaluation is critical to preserving a functioning access. We hypothesized that a risk score using measurements obtained from the Vasc-Alert surveillance device could be used to predict subsequent interventions.
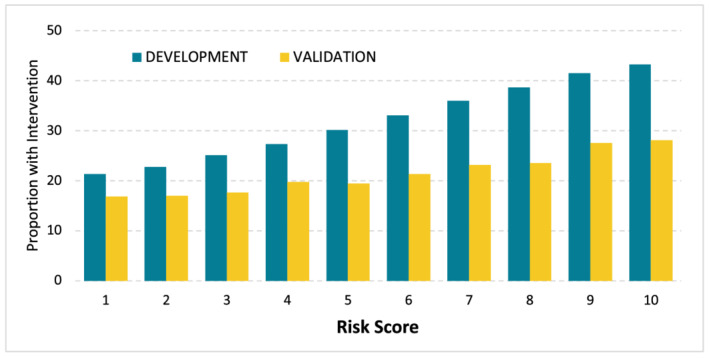
Methods: Measurement of five factors over the preceding 28 days from 1.46 million hemodialysis treatments (6163 patients) were used to develop a score associated with interventions over the subsequent 60 days. The score was validated in a separate dataset of 298,620 treatments (2641 patients).
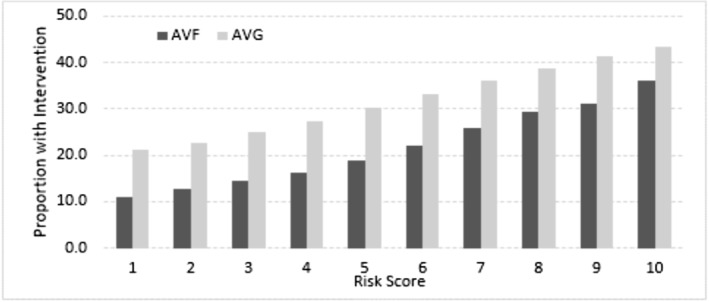
Results: Interventions in arteriovenous fistulae (AVF; n = 4125) were much more common in those with the highest score (36.2%) than in those with the lowest score (11.0). The score also was strongly associated with interventions in patients with an arteriovenous graft (AVG; n = 2,038; 43.2% vs. 21.1%). There was excellent agreement in the Validation datasets for AVF (OR = 2.67 comparing the highest to lowest score) and good agreement for AVG (OR = 1.92).
Conclusions: This simple risk score based on surveillance data may be useful for prioritizing patients for physical examination and potentially early referral for intervention.
© 2021 The Authors. Seminars in Dialysis published by Wiley Periodicals LLC.
Figures




References
-
- Riella MC, Roy‐Chaudhury P. Vascular access in haemodialysis: strengthening the Achilles' heel. Nat Rev Nephrol. 2013;9(6):348‐357. - PubMed
-
- Thamer M, Lee TC, Wasse H, et al. Medicare Costs Associated With Arteriovenous Fistulas Among US Hemodialysis Patients. Am J Kidney Dis. 2018. Jul;72(1):10‐18. - PubMed
-
- Manns B, Tonelli M, Yilmaz S, et al. Establishment and maintenance of vascular access in incident hemodialysis patients: a prospective cost analysis. JASN. 2005;16(1):201‐209. - PubMed
-
- Sands JJ. Vascular access monitoring improves outcomes. Blood Purif. 2005;23(1):45‐49. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
