

[Evaluation of cancelled emergency physician missions and patient handovers in the area of Innsbruck : Retrospective assessment of physician-staffed emergency medical service cancellations and handovers from the emergency physician to the emergency medical service in 2017 and 2018]
- PMID: 34643756
- PMCID: PMC8986753
- DOI: 10.1007/s00101-021-01046-y
[Evaluation of cancelled emergency physician missions and patient handovers in the area of Innsbruck : Retrospective assessment of physician-staffed emergency medical service cancellations and handovers from the emergency physician to the emergency medical service in 2017 and 2018]
Abstract
Background: Human and vehicle resource management indicates a good emergency medical system (EMS). Frequently, an emergency medical technician (EMT) is the first responder to the emergency, which negates the necessity for an emergency physician (EP) and is just as sensible as handing over a stable patient to the EMT for transport to the hospital. The Austrian EMS is utilized by EMTs, in cases of potential life-threatening emergencies the dispatch center dispatches an additional team with an on-board EP. During the years 2017-2018 nearly every fifth EP mission in Innsbruck (including surrounding areas) ended in a cancellation. The numbers of patient handovers from EP to EMT are slightly lower with mission cancellations resulting in every fourth patient. Therefore, due to the high number of cancellations and handovers evaluated in this study, the findings suggest that there is a potential need to re-evaluate procedures. The re-evaluation of these procedures could determine whether these cancellations/handovers were justified or if an over hasty decision making was at fault. All cases considered in this study were from the Innsbruck and Telfs EP bases between 1 January 2017 and 13 December 2018.
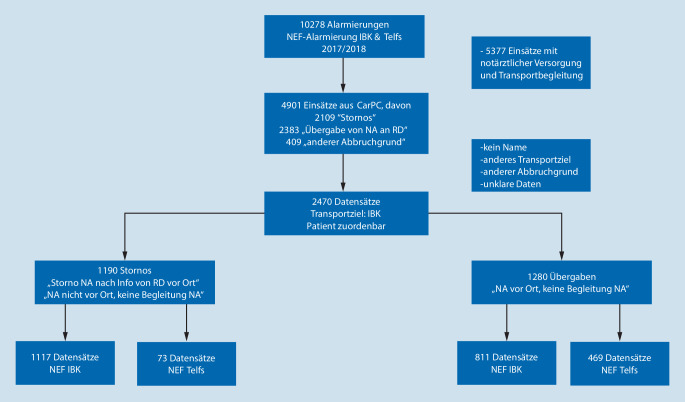
Methods: Out of a total of 96,908 emergency dispatches, there were 2470 cancellation/handover occurrences. These occurrences consisted of 1190 cancellations and 1280 patient handovers from the EP to the EMT. Patients who were transferred to the University Hospital Innsbruck were included in these figures. The protocols of the emergency dispatches have been filtered from the so-called CarPC. They have subsequently been grouped into cancellation and handover categories. The clinical diagnoses of the patients with inpatient treatment were evaluated from the hospital information system (KIS) of the University Hospital Innsbruck. This was done with the help of the so-called emergency physician indications catalogue of the German Medical Council. The diagnosis was documented in the hospital information system. The emergency protocols from the EMTs were also evaluated retrospectively. The Innsbruck based EP patients are hospitalized in the Innsbruck Hospital due their geographical position. When there is no need for a specific intervention the patients of the EPs based in Telfs are transferred to a local hospital. When a specific intervention is necessary, patient care must be provided by the University Hospital Innsbruck. Due to the privacy practices of the Innsbruck Medical University "vote of ethics" only the data of patients transferred to the Innsbruck Clinic can be evaluated. The information provided from the EPs based in Innsbruck was exclusively from the University Hospital Innsbruck's anesthesiologists. The physicians from the Telfs EP base are of mixed medical specialities. All of them, however, have an emergency medical physician diploma, in addition to the ius practicandi. Lastly, there are no EPs in Innsbruck or Telfs, who have any special obligations during their duty.
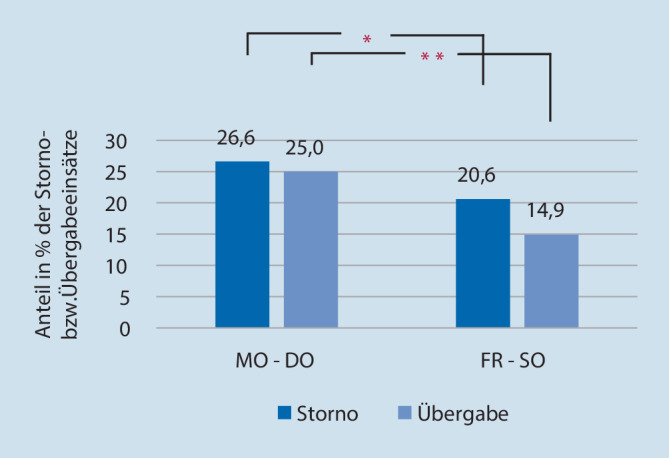
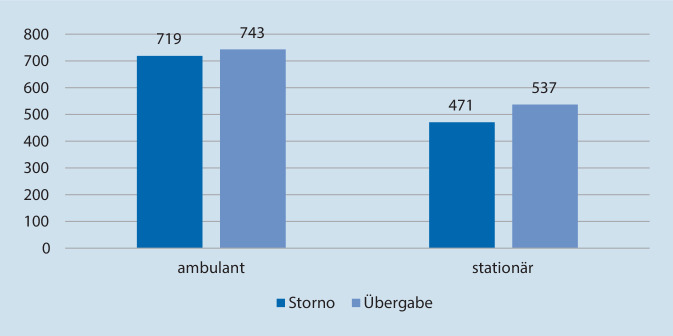
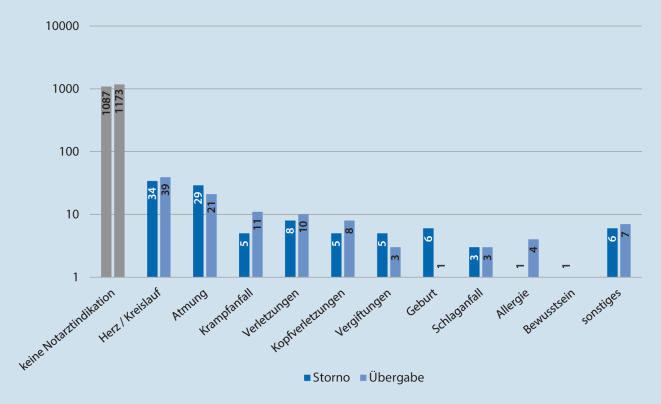
Results: The results show that in 210 cases (8.5%) the indications for the EP, based on the emergency physician indications catalogue of the German Medical Council were given. Also, 8.7% of all cancellations and 8.4% of patient handovers were not justified. Patients with emergency indications had a longer hospitalization. The EP base EMS Innsbruck had more cancellations than the EP base EMS Telfs. The EMS Innsbruck also had more cancellations than patient handovers. Conversely, the EMS Telfs had more patient handovers than cancellations. On the weekends between 6:00 pm and 6:00 am there were less cancellations and handovers from both EP bases. The documentation from the EMT protocols was incomplete in 284 cancellations (23.9% of the cancellations) and 339 handovers (26.5% of the handovers), 35 patients after cancellations (2.9%), 35 patients after handovers (2.7%) needed intensive care treatment, 20 patients after cancellations (1.7% of all cancellations), and 24 patients after handovers (1.9% of all handovers) who needed intensive care treatment had a critical diagnosis. In 40 cases of patient handovers, the EP was alerted to another emergency follow-up within 10 min.
Conclusion: In Austria, the introduction of a standardized emergency indication checklist might help dispatch centers to provide a more accurate dispatch as well as all EMS team members. Furthermore, a better traceability system (according to EP cancellations and patient handovers from the EP to the EMT) could be achieved. The documentation requirements should be more precise by all members of the EMT staff, not only for the legal aspects but also for improving the overall management quality. Intense education and training as well as diagnosis feedbacks could help to reduce the number of risky cancellations/patient handovers.
Zusammenfassung: HINTERGRUND: Die Qualität eines Rettungssystems zeichnet sich auch durch den effizienten Einsatz seiner personellen und Fahrzeugressourcen aus. So können im berechtigten Fall Stornierungen des anfahrenden Notarztes durch den Rettungsdienst (RD) ebenso sinnvoll sein wie Übergaben des stabilen Patienten an den RD. Aufgrund der hohen Zahlen solcher Storno- und Übergabeeinsätze evaluiert diese Studie diese Entscheidungen retrospektiv und zeigt evtl. Auffälligkeiten auf. Studienkollektiv waren die 10.278 Notarztalarmierungen der beiden Notarzteinsatzfahrzeuge (NEF) Innsbruck Stadt (städtisch) und Telfs (ländlich) der Jahre 2017 und 2018.
Methode: Der Patientenzustand sowie die Rettungsdienstdokumentation wurden beurteilt und die Notarztindikation retrospektiv anhand der klinischen Aufnahmediagnosen im Abgleich mit dem Notarztindikationskataloges der Deutschen Bundesärztekammer (NIKDBÄK) anhand vorgegebener Kriterien wie eingegebener Vitalparameter und/oder des Notfallgeschehens bewertet.
Ergebnisse: Im zweijährigen Studienzeitraum ergaben sich 2470 relevante Datensätze, davon 1190 Storno- und 1280 Übergabeeinsätze mit gesamt 210 Einsätzen (8,5 %) mit Notarztindikation laut NIKDBÄK. Am NEF Innsbruck fanden mehr Stornierungen statt, und es kam zu mehr Storno- als Übergabeeinsätzen, umgekehrt dazu am NEF Telfs zu mehr Übergabe- als Stornoeinsätzen. An Wochenenden fanden nachts weniger Storno- und Übergabeeinsätze statt. In 284 Protokollen bei Stornierungen (23,9 %) und 339 Protokollen bei Übergaben (26,5 %) war die Dokumentation der Sanitäterprotokolle unvollständig. Patienten mit gegebener Notarztindikation laut NIKDBÄK mussten länger stationär behandelt werden. 35 Patienten nach Storno- (2,9 %) und 35 Patienten nach Übergabeeinsätzen (2,7 %) mussten auf einer Intensivstation aufgenommen werden. Bei den Intensivbehandlungen wurde bei 20 Patienten (1,7 % der Stornoeinsätze) nach einem Stornoeinsatz eine kritische Aufnahmediagnose festgestellt bzw. bei 24 Patienten (1,9 % der Übergabeeinsätze) nach einem Übergabeeinsatz. Bei 40 (3,1 %) Übergabeeinsätzen vom Notarzt an den Rettungsdienst kam es innerhalb von 10 min nach Eintreffen des Notarztes zu einem Folgeeinsatz.
Schlussfolgerung: Die Einführung eines eigenen standardisierten Notfallindikationskataloges für Österreich erscheint als Vorgabe für Leitstellen und Rettungsdienstpersonal sinnvoll. Storno- und Übergabeentscheidungen müssen sorgsam getroffen werden und sollten QM-gesichert evaluiert werden. Der Dokumentationspflicht im Rettungswesen muss vermehrte Aufmerksamkeit gewidmet werden. Durch intensivere Aus- und Fortbildungen sowie Diagnosefeedbacks könnte die Anzahl an unberechtigten bzw. risikobehafteten Storno‑/Übergabeeinsätzen vermindert werden.
Keywords: Documentation; Emergency physician cancellation; Indication checklist; Patient handovers; Quality control.
© 2021. The Author(s).

References
-
- AGNNW Arbeitsgemeinschaft Notärzte in NRW (2020) Handbuch Notfallmedizin – Notfallmedizinisches Kompendium der Arbeitsgemeinschaft Notärzte in NRW. Eigenverlag AGNNW, Nordrhein-Westfalen, S. 43–44. https://www.agnnw.de/?p=2179. Zugegriffen: 10. Febr. 2021
-
- Bayerische Landesärztekammer (2021) Notfallmedizin. https://www.blaek.de/weiterbildung/qualifikationen-nach-der-weiterbildun.... Zugegriffen: 6. Aug. 2021
-
- Bernar B, Kuhn P, Kaiser H, et al. Notfallmedizinischer Kennzahlen- und Benchmarkbericht Tirol. Notfall Rettungsmed. 2016;19:638–645. doi: 10.1007/s10049-016-0249-3. - DOI
-
- Bollinger M, Roessler M, Russo S. Inzidenz invasiver ärztlicher Maßnahmen im Rettungsdienst. Notfall Rettungsmed. 2015;18:215–221. doi: 10.1007/s10049-015-0001-4. - DOI
-
- Burkowski M, Halmich M. SanG Sanitätergesetz mit San-AV und SanAFV. Wien: NWV; 2016.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
