

Brain-lung interactions and mechanical ventilation in patients with isolated brain injury
- PMID: 34645485
- PMCID: PMC8512596
- DOI: 10.1186/s13054-021-03778-0
Brain-lung interactions and mechanical ventilation in patients with isolated brain injury
Abstract
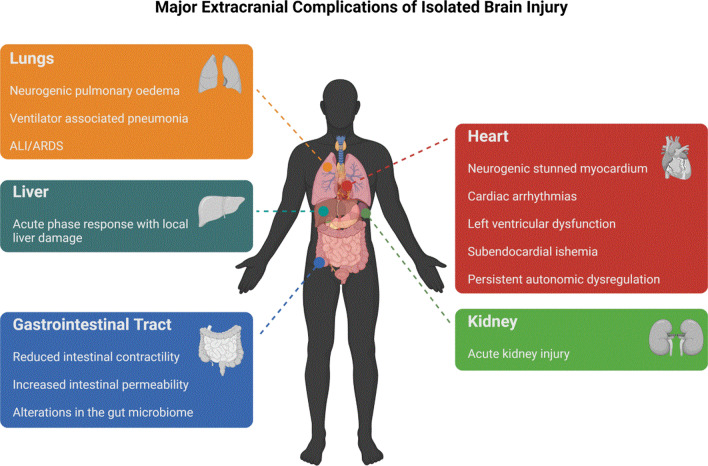
During the last decade, experimental and clinical studies have demonstrated that isolated acute brain injury (ABI) may cause severe dysfunction of peripheral extracranial organs and systems. Of all potential target organs and systems, the lung appears to be the most vulnerable to damage after brain injury (BI). The pathophysiology of these brain-lung interactions are complex and involve neurogenic pulmonary oedema, inflammation, neurodegeneration, neurotransmitters, immune suppression and dysfunction of the autonomic system. The systemic effects of inflammatory mediators in patients with BI create a systemic inflammatory environment that makes extracranial organs vulnerable to secondary procedures that enhance inflammation, such as mechanical ventilation (MV), surgery and infections. Indeed, previous studies have shown that in the presence of a systemic inflammatory environment, specific neurointensive care interventions-such as MV-may significantly contribute to the development of lung injury, regardless of the underlying mechanisms. Although current knowledge supports protective ventilation in patients with BI, it must be born in mind that ABI-related lung injury has distinct mechanisms that involve complex interactions between the brain and lungs. In this context, the role of extracerebral pathophysiology, especially in the lungs, has often been overlooked, as most physicians focus on intracranial injury and cerebral dysfunction. The present review aims to fill this gap by describing the pathophysiology of complications due to lung injuries in patients with a single ABI, and discusses the possible impact of MV in neurocritical care patients with normal lungs.
Keywords: Acute respiratory distress syndrome; Brain damage; Brain–lung interactions; Inflammation; Mechanical ventilation; Ventilator induced lung injury.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- McDonald SJ, et al. Beyond the brain: peripheral interactions after traumatic brain injury. J Neurotrauma. 2020;37(5):770–781. - PubMed
-
- Brain Trauma F, et al. Guidelines for the management of severe traumatic brain injury. XIV Hyperventilation. J Neurotrauma. 2007;24(Suppl 1):S87–90. - PubMed
-
- Robba C, et al. Extracranial complications after traumatic brain injury: targeting the brain and the body. Curr Opin Crit Care. 2020;26(2):137–146. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
