

Prevalence and determinants of serum antibodies to SARS-CoV-2 in the general population of the Gardena valley
- PMID: 34645534
- PMCID: PMC8387688
- DOI: 10.1017/S0950268821001886
Prevalence and determinants of serum antibodies to SARS-CoV-2 in the general population of the Gardena valley
Abstract
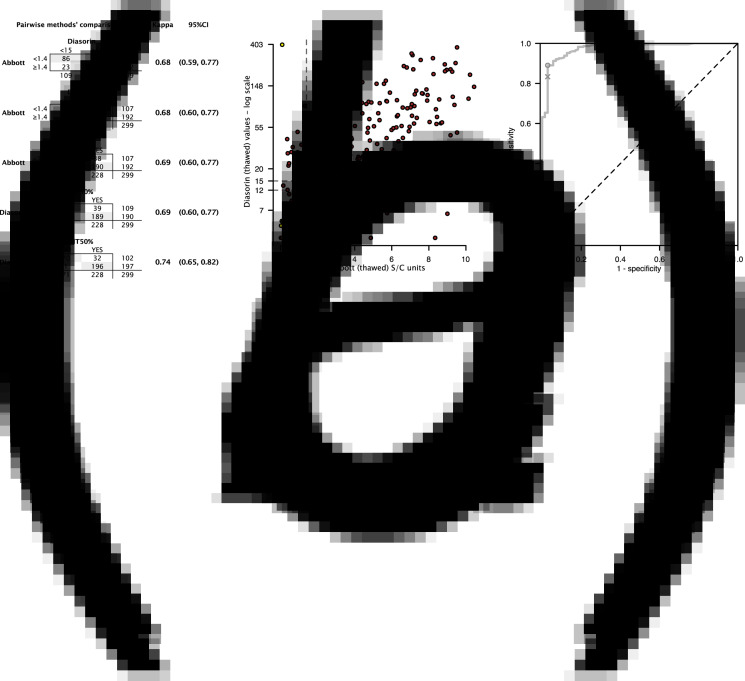
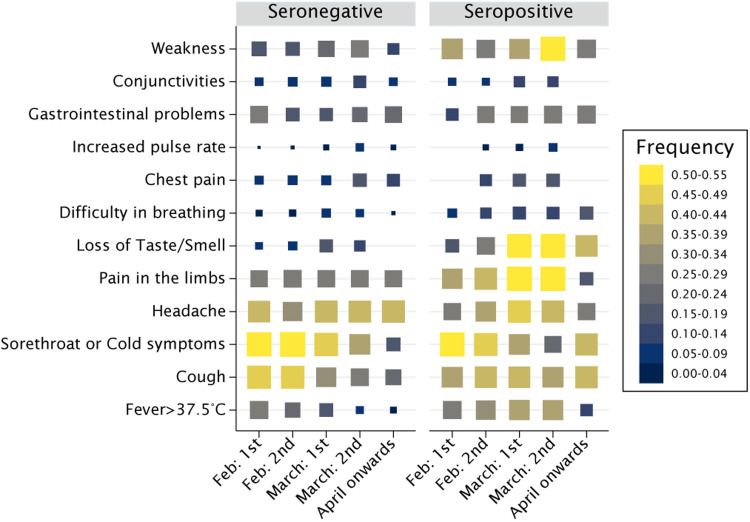
Estimating the spread of SARS-CoV-2 infection in communities is critical. We surveyed 2244 stratified random sample community members of the Gardena valley, a winter touristic area, amidst the first expansion phase of the COVID-19 pandemic in Europe. We measured agreement between Diasorin and Abbott serum bioassay outputs and the Abbott optimal discriminant threshold of serum neutralisation titres with recursive receiver operating characteristic curve. We analytically adjusted serum antibody tests for unbiased seroprevalence estimate and analysed the determinants of infection with non-response weighted multiple logistic regression. SARS-CoV-2 seroprevalence was 26.9% (95% CI 25.2-28.6) by June 2020. The bioassays had a modest agreement with each other. At a lower threshold than the manufacturer's recommended level, the Abbott assay reflected greater discrimination of serum neutralisation capacity. Seropositivity was associated with place and economic activity, not with sex or age. Symptoms like fever and weakness were age-dependent. SARS-CoV-2 mitigation strategies should account for context in high prevalence areas.
Keywords: COVID-19; Coronavirus; SARS-CoV-2; neutralising antibodies; prevalence.
Conflict of interest statement
None.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
