

Nomogram Incorporating Contrast-Enhanced Ultrasonography Predicting Time to the Development of Castration-Resistant Prostate Cancer
- PMID: 34646064
- PMCID: PMC8504687
- DOI: 10.1177/11795549211049750
Nomogram Incorporating Contrast-Enhanced Ultrasonography Predicting Time to the Development of Castration-Resistant Prostate Cancer
Abstract
Background: It is valuable to predict the time to the development of castration-resistant prostate cancer (CRPC) in patients with advanced prostate cancer (PCa). This study aimed to build and validate a nomogram incorporating the clinicopathologic characteristics and the parameters of contrast-enhanced ultrasonography (CEUS) to predict the time to CRPC after androgen deprivation therapy (ADT).
Methods: Patients with PCa were divided into the training (n = 183) and validation cohorts (n = 37) for nomogram construction and validation. The clinicopathologic characteristics and CEUS parameters were analyzed to determine the independent prognosis factors and serve as the basis of the nomogram to estimate the risk of 1-, 2-, and 3-year progress to CRPC.
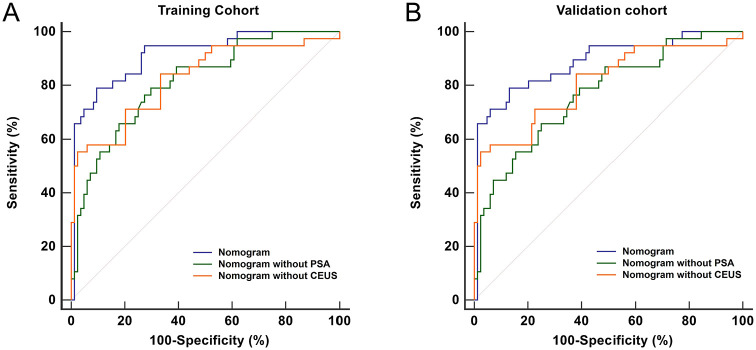
Results: T stage, distant metastasis, Gleason score, area under the curve (AUC), prostate-specific antigen (PSA) nadir, and time to PSA nadir were the independent predictors of CRPC (all P < 0.05). Three nomograms were built to predict the time to CRPC. Owing to the inclusion of CEUS parameter, the discrimination of the established nomogram (C-index: 0.825 and 0.797 for training and validation datasets) was improved compared with the traditional prediction model (C-index: 0.825 and 0.797), and when it excluded posttreatment PSA, it still obtained an acceptable discrimination (C-index: 0.825 and 0.797).
Conclusions: The established nomogram including regular prognostic indicators and CEUS obtained an improved accuracy for the prediction of the time to CRPC. It was also applicable for early prediction of CRPC when it excluded posttreatment PSA, which might be helpful for individualized diagnosis and treatment.
Keywords: Castration-resistant prostate cancer; androgen deprivation therapy; contrast-enhanced ultrasonography; nomogram; prostate-specific antigen.
© The Author(s) 2021.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures





Similar articles
-
[Predictive factor analysis of time to progression of castration-resistant prostate cancer after androgen deprivation therapy].Beijing Da Xue Xue Bao Yi Xue Ban. 2017 Aug 18;49(4):657-662. Beijing Da Xue Xue Bao Yi Xue Ban. 2017. PMID: 28816284 Chinese.
-
Prostate-specific antigen kinetic profiles during androgen deprivation therapy as prognostic factors in castration-resistant prostate cancer.Urol Oncol. 2015 May;33(5):203.e1-9. doi: 10.1016/j.urolonc.2015.01.017. Epub 2015 Feb 26. Urol Oncol. 2015. PMID: 25726498
-
A simple prognostic model involving prostate-specific antigen, alkaline phosphatase and albumin for predicting the time required to progress to castration-resistant prostate cancer in patients who received androgen deprivation therapy.Int Urol Nephrol. 2017 Jan;49(1):61-67. doi: 10.1007/s11255-016-1456-z. Epub 2016 Nov 11. Int Urol Nephrol. 2017. PMID: 27837416
-
The Importance of Time to Prostate-Specific Antigen (PSA) Nadir after Primary Androgen Deprivation Therapy in Hormone-Naïve Prostate Cancer Patients.J Clin Med. 2018 Dec 18;7(12):565. doi: 10.3390/jcm7120565. J Clin Med. 2018. PMID: 30567361 Free PMC article. Review.
-
EAU guidelines on prostate cancer. Part II: Treatment of advanced, relapsing, and castration-resistant prostate cancer.Eur Urol. 2011 Apr;59(4):572-83. doi: 10.1016/j.eururo.2011.01.025. Epub 2011 Jan 25. Eur Urol. 2011. PMID: 21315502
Cited by
-
Effects of miR-103a-3p Targeted Regulation of TRIM66 Axis on Docetaxel Resistance and Glycolysis in Prostate Cancer Cells.Front Genet. 2022 Feb 8;12:813793. doi: 10.3389/fgene.2021.813793. eCollection 2021. Front Genet. 2022. PMID: 35211152 Free PMC article.
-
The combined value of mpUS and mpMRI-TRUS fusion for the diagnosis of clinically significant prostate cancer.Cancer Imaging. 2022 Oct 18;22(1):60. doi: 10.1186/s40644-022-00498-8. Cancer Imaging. 2022. PMID: 36258247 Free PMC article.
-
Predictive Models for Assessing Patients' Response to Treatment in Metastatic Prostate Cancer: A Systematic Review.Eur Urol Open Sci. 2024 Apr 4;63:126-135. doi: 10.1016/j.euros.2024.03.012. eCollection 2024 May. Eur Urol Open Sci. 2024. PMID: 38596781 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
