

Is there any room for PD-1 inhibitors in combination with platinum-based chemotherapy as frontline treatment of extensive-stage small cell lung cancer? A systematic review and meta-analysis with indirect comparisons among subgroups and landmark survival analyses
- PMID: 34646363
- PMCID: PMC8504650
- DOI: 10.1177/17588359211018018
Is there any room for PD-1 inhibitors in combination with platinum-based chemotherapy as frontline treatment of extensive-stage small cell lung cancer? A systematic review and meta-analysis with indirect comparisons among subgroups and landmark survival analyses
Abstract
Background: The addition of PD-L1 inhibitors to platinum-based chemotherapy (CT) has newly received United States Food and Drug Administration (FDA) approval in extensive stage-small cell lung cancer (ES-SCLC). PD-1 agents similarly improved survival rates, even if not yet supported by international regulatory agencies. The current work aims to assess different efficacy and safety profiles among chemoimmunotherapy plus immuno-oncology (CT+IO) approaches according to different immune checkpoint inhibitor (ICI) subtypes.
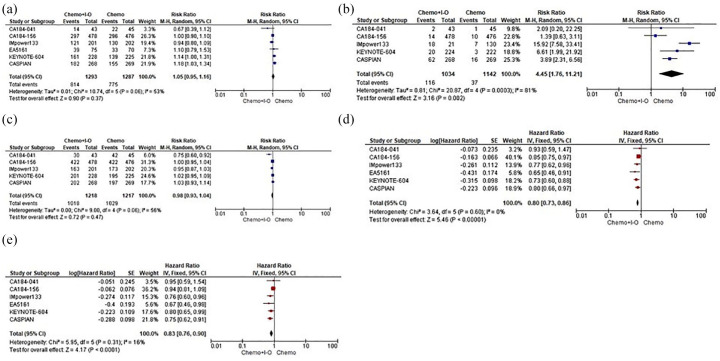
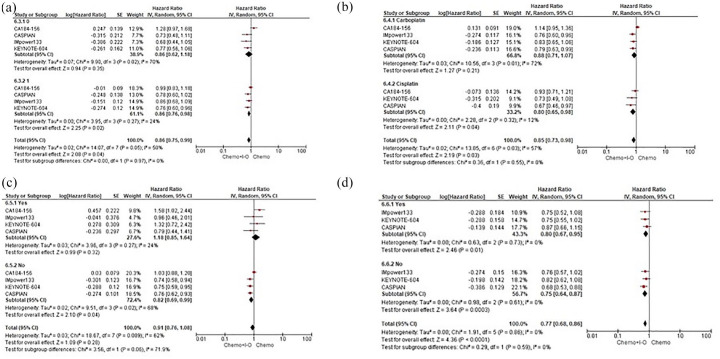
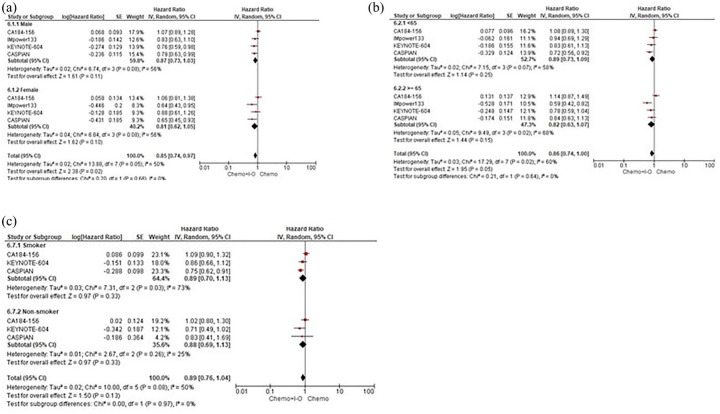
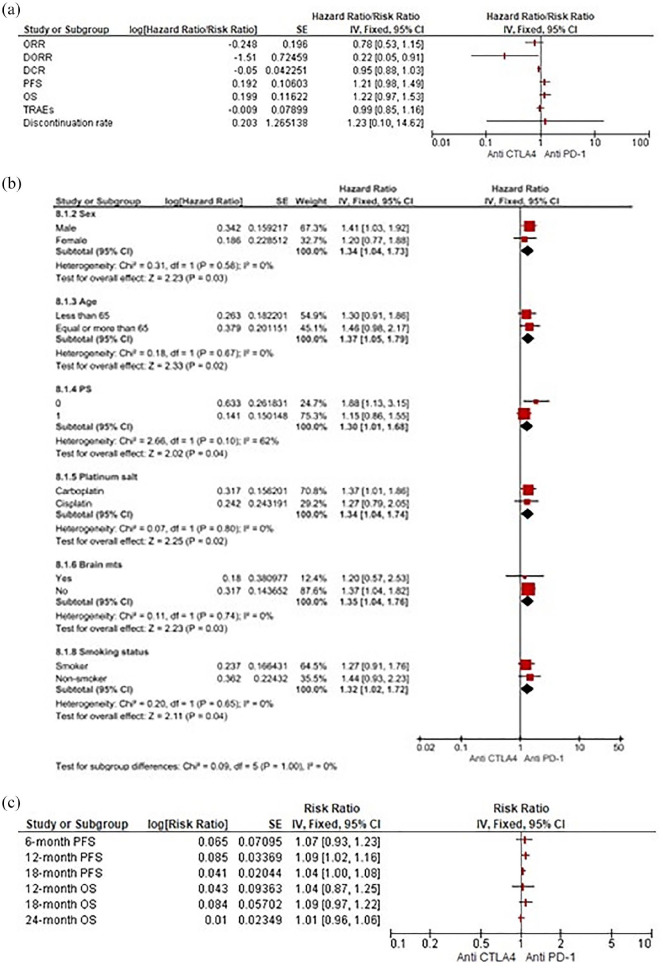
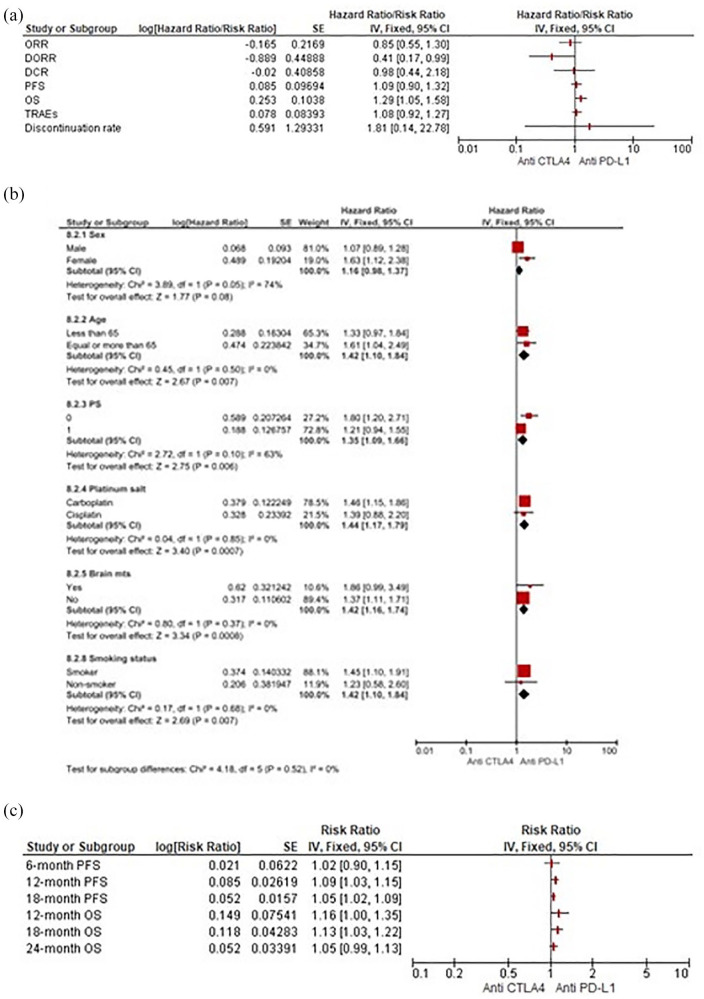
Material & methods: We included in our meta-analysis six first-line randomised controlled trials (RCTs) comparing the association of single-agent ICI with CT versus CT alone in ES-SCLC. Pooled hazard ratios (HRs) and risk ratios (RRs) for progression-free survival (PFS), overall survival (OS), objective response rates (ORR), 12-month duration of response rate (DORR), disease control rate (DCR), treatment-related adverse events (TRAEs) and discontinuation rates (DRs) were obtained. Moreover, we performed indirect comparisons according to ICI subtypes, also among subgroups and landmark survival analyses.
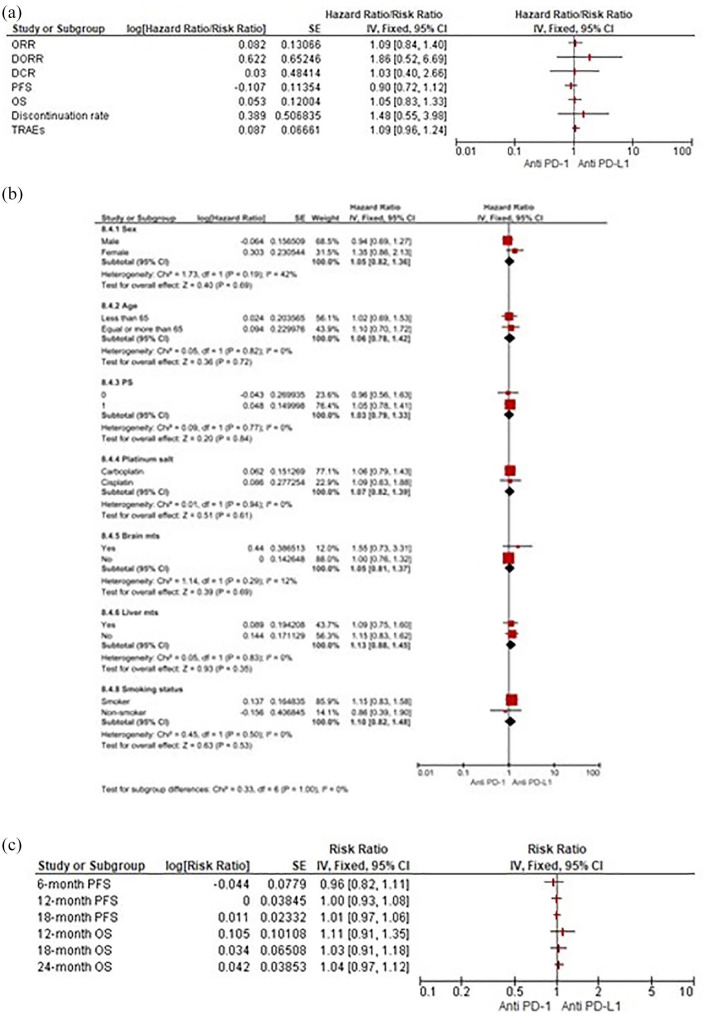
Results: Although no ORR benefit was observed, our results showed how CT+IO significantly improved DORR, resulting in improved PFS and OS with no differences in TRAEs; however, CT+IO led to a significant increase in DR. Interestingly, an Eastern Cooperative Oncology Group performance status (ECOG PS) of 1, the use of cisplatin, and the absence of brain metastases seem to be associated with a survival gain using CT+IO in ES-SCLC. Indirect comparisons suggested a slight advantage in favour of programmed cell death-1 (PD-1) and programmed death ligand 1 (PD-L1) over anti-CTLA-4 agents in terms of efficacy with no additional safety concerns. No further differences were observed between PD-1 and PD-L1 inhibitors among subgroups and landmark survival analyses with benefit trends towards anti-PD-1 in terms of DORR and DR.
Conclusion: While confirming a survival advantage of CT+IO in selected patients, these results suggested the association of PD-1 inhibitors with CT as a viable option for novel therapeutic approaches in the frontline management of ES-SCLC. Further trials evaluating anti-CTLA-4 agents should be carefully studied in biomarker-selected patients.
Keywords: ES-SCLC; PD-L1/PD-1 inhibitors; chemo-immunotherapy; indirect comparison; meta-analysis.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: A. Russo reports personal fees from Bristol, Pfizer, Bayer, Kyowa Kirin, Ambrosetti for advisory board activity; speaker honorarium from Roche Diagnostics. The remaining authors declare no potential conflicts of interest.
Figures

References
-
- Govindan R, Page N, Morgensztern D, et al.. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol 2006; 24: 4539–4544. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin 2020; 70: 7–30. - PubMed
-
- Nicholson AG, Chansky K, Crowley J, et al.. The international association for the study of lung cancer lung cancer staging project: proposals for the revision of the clinical and pathologic staging of small cell lung cancer in the forthcoming eighth edition of the TNM classification for lung cancer. J Thorac Oncol 2016; 11: 300–311. - PubMed
-
- Kauffmann-Guerrero D, Kahnert K, Syunyaeva Z, et al.. Pretherapeutic inflammation predicts febrile neutropenia and reduced progression-free survival after first-line chemotherapy in SCLC. Oncol Res Treat 2018; 41: 506–512. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
