

Comparison of Dosimetric Benefits of Three Precise Radiotherapy Techniques in Nasopharyngeal Carcinoma Patients Using a Priority-Classified Plan Optimization Model
- PMID: 34646757
- PMCID: PMC8504456
- DOI: 10.3389/fonc.2021.646584
Comparison of Dosimetric Benefits of Three Precise Radiotherapy Techniques in Nasopharyngeal Carcinoma Patients Using a Priority-Classified Plan Optimization Model
Abstract
Introduction: Although intensity-modulated radiotherapy (IMRT), volumetric-modulated arc therapy (VMAT) and tomotherapy (TOMO) are broadly applied for nasopharyngeal carcinoma (NPC), the best technique remains unclear. Therefore, this study was conducted to address this issue.
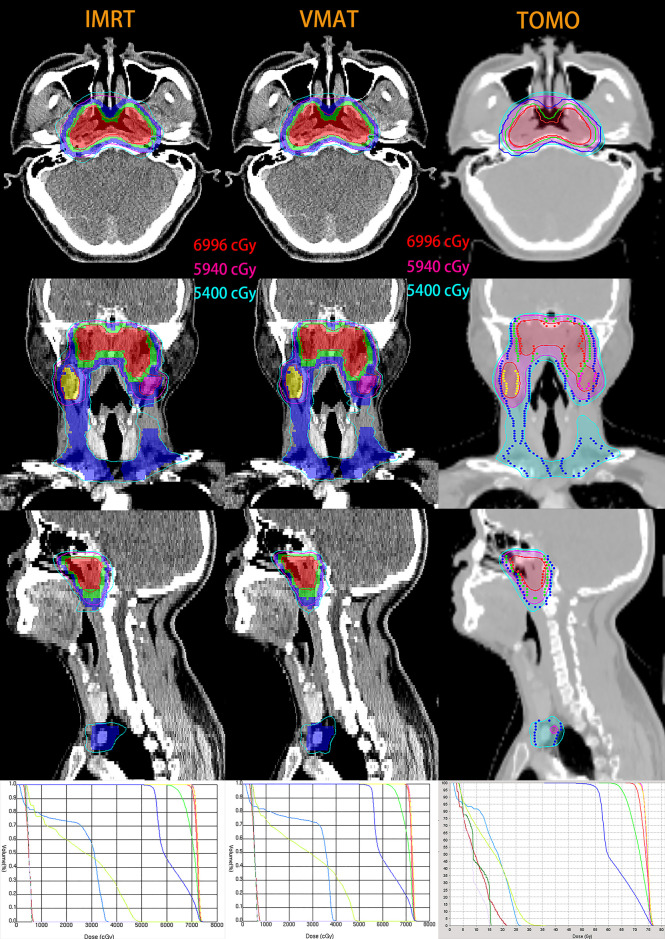
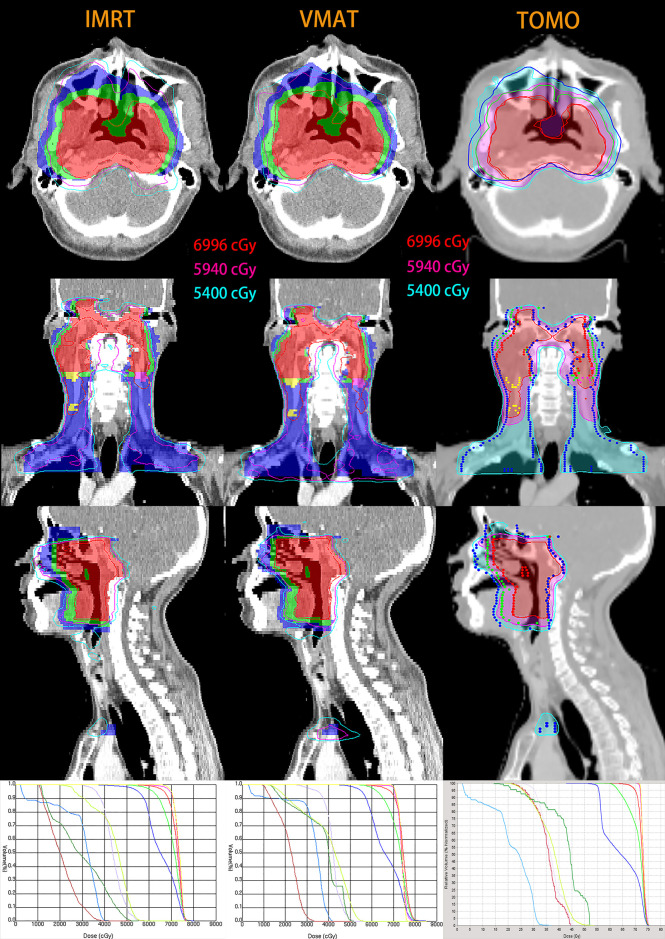
Methods: The priority-classified plan optimization model was applied to IMRT, VMAT and TOMO plans in forty NPC patients according to the latest international guidelines. And the dosimetric parameters of planning target volumes (PTVs) and organs at risk (OARs) were compared among these three techniques. The Friedman M test in SPSS software was applied to assess significant differences.
Results: The median PGTVnx coverage of IMRT was the lowest (93.5%, P < 0.001) for all T categories. VMAT was comparable to TOMO in OARs clarified as priority I and II, and both satisfied the prescribed requirement. IMRT resulted in a relatively high dose for V25 and V30. Interestingly, subgroup analysis showed that the median PTV coverage of the three techniques was no less than 95% in the early T stage. The heterogeneity index (HI) of PGTVnx in VMAT was better than that in IMRT (P = 0.028). Compared to TOMO, VMAT showed a strong ability to protect eyesight and decrease low-dose radiation volumes. In the advanced T stage subgroup, TOMO numerically achieved the highest median PGTVnx coverage volume compared with VMAT and IMRT (93.61%, 91% and 90%, respectively). The best CI and HI of PCTV-1 were observed in TOMO. Furthermore, TOMO was better than VMAT for sparing the brain stem, spinal cord and temporal lobes (all P < 0.05). However, the median V5, V10, V15, V20 and V25 were significantly higher with TOMO than with VMAT (all P < 0.05).
Conclusion: In the early T stage, VMAT provides a similar dose coverage and protection of OARs to IMRT, and there are no obvious advantages to choosing TOMO for NPC patients in the early T stage. TOMO may be recommended for patients in the advanced T stage due as it provides the largest dose coverage of PGTVnx and the best protection of the brain stem, spinal cord and temporal lobes. Additionally, more randomized clinical trials are needed for further clarification.
Keywords: dosimetry; intensity-modulated radiotherapy; nasopharyngeal carcinoma; tomotherapy; volumetric-modulated arc therapy.
Copyright © 2021 Wang, Qin, Cao, Xu, Yan, Zhu, Wu, Xu, Zhu, Jiang, Li and Xiong.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer [YT] declared a shared affiliation with one of the authors [WJ] to the handling editor at the time of review.
Figures
Similar articles
-
Tomotherapy as a neoadjuvant treatment for locally advanced esophageal cancer might increase bone marrow toxicity in comparison with intensity-modulated radiotherapy and volumetric-modulated arc therapy.Med Dosim. 2020 Spring;45(1):e6-e12. doi: 10.1016/j.meddos.2019.05.001. Epub 2019 Jun 5. Med Dosim. 2020. PMID: 31176536
-
[Dosimetric comparison of the helical tomotherapy, intensity-modulated radiotherapy and volumetric-modulated arc therapy in radical radiotherapy for esophageal cancer].Zhonghua Yi Xue Za Zhi. 2019 Nov 5;99(41):3260-3265. doi: 10.3760/cma.j.issn.0376-2491.2019.41.012. Zhonghua Yi Xue Za Zhi. 2019. PMID: 31694123 Chinese.
-
Dosimetry comparison with helical tomotherapy, volumetric modulated arc therapy, and intensity-modulated radiotherapy for grade II gliomas: A single‑institution case series.Open Life Sci. 2023 Feb 10;18(1):20220550. doi: 10.1515/biol-2022-0550. eCollection 2023. Open Life Sci. 2023. PMID: 36820205 Free PMC article.
-
Compared planning dosimetry of TOMO, VMAT and IMRT in rectal cancer with different simulated positions.Oncotarget. 2017 Jun 27;8(26):42020-42029. doi: 10.18632/oncotarget.14923. Oncotarget. 2017. PMID: 28159930 Free PMC article.
-
Volumetric-modulated arc therapy for the treatment of a large planning target volume in thoracic esophageal cancer.J Appl Clin Med Phys. 2013 May 6;14(3):4269. doi: 10.1120/jacmp.v14i3.4269. J Appl Clin Med Phys. 2013. PMID: 23652258 Free PMC article.
Cited by
-
Helical tomotherapy and two types of volumetric modulated arc therapy: dosimetric and clinical comparison for several cancer sites.Radiol Phys Technol. 2023 Jun;16(2):272-283. doi: 10.1007/s12194-023-00716-3. Epub 2023 Apr 21. Radiol Phys Technol. 2023. PMID: 37084071
-
Volumetric modulated arc therapy versus tomotherapy for late T-stage nasopharyngeal carcinoma.Front Oncol. 2022 Aug 8;12:961781. doi: 10.3389/fonc.2022.961781. eCollection 2022. Front Oncol. 2022. PMID: 36003797 Free PMC article.
-
Dosimetric Comparison of Noncoplanar VMAT Without Rotating the Patient Couch Versus Conventional Coplanar/Noncoplanar VMAT for Head and Neck Cancer: First Report of Dynamic Swing Arc.Adv Radiat Oncol. 2024 Dec 30;10(3):101706. doi: 10.1016/j.adro.2024.101706. eCollection 2025 Mar. Adv Radiat Oncol. 2024. PMID: 39911721 Free PMC article.
-
Impact of monitor unit optimization in volumetric modulated arc therapy planning for nasopharyngeal carcinoma.PLoS One. 2025 Jun 25;20(6):e0327153. doi: 10.1371/journal.pone.0327153. eCollection 2025. PLoS One. 2025. PMID: 40561140 Free PMC article.
-
Optimizing stereotactic ablative body radiotherapy for ultra-central lung lesions: a comparative dosimetric analysis.Radiat Oncol. 2025 Jun 18;20(1):103. doi: 10.1186/s13014-025-02675-y. Radiat Oncol. 2025. PMID: 40533770 Free PMC article.
References
-
- Shanmugaratnam K. Nasopharyngeal Carcinoma: Epidemiology, Histopathology and Aetiology. Ann Acad Med Singapore (1980) 9(3):289–95. - PubMed
-
- Yu MC. Nasopharyngeal Carcinoma: Epidemiology and Dietary Factors. IARC Sci Publ (1991) 105):39–47. - PubMed
-
- Luo WJ, Zou WQ, Liang SB, Chen L, Zhou GQ, Peng H, et al. . Combining Tumor Response and Personalized Risk Assessment: Potential for Adaptation of Concurrent Chemotherapy in Locoregionally Advanced Nasopharyngeal Carcinoma in the Intensity-Modulated Radiotherapy Era. Radiother Oncol (2020) 155:56–64. doi: 10.1016/j.radonc.2020.10.005 - DOI - PubMed
-
- Liu LT, Liang YJ, Guo SS, Mo HY, Guo L, Wen YF, et al. . Induction Chemotherapy Followed by Radiotherapy Versus Concurrent Chemoradiotherapy in the Treatment of Different Risk Locoregionally Advanced Nasopharyngeal Carcinoma. Ther Adv Med Oncol (2020) 12:1758835920928214. doi: 10.1177/1758835920928214 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources