

Exhausting T Cells During HIV Infection May Improve the Prognosis of Patients with COVID-19
- PMID: 34646783
- PMCID: PMC8502810
- DOI: 10.3389/fcimb.2021.564938
Exhausting T Cells During HIV Infection May Improve the Prognosis of Patients with COVID-19
Abstract
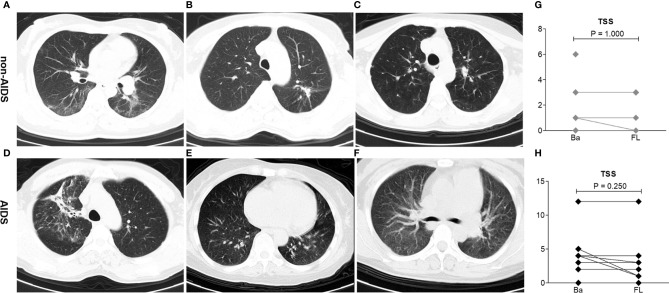
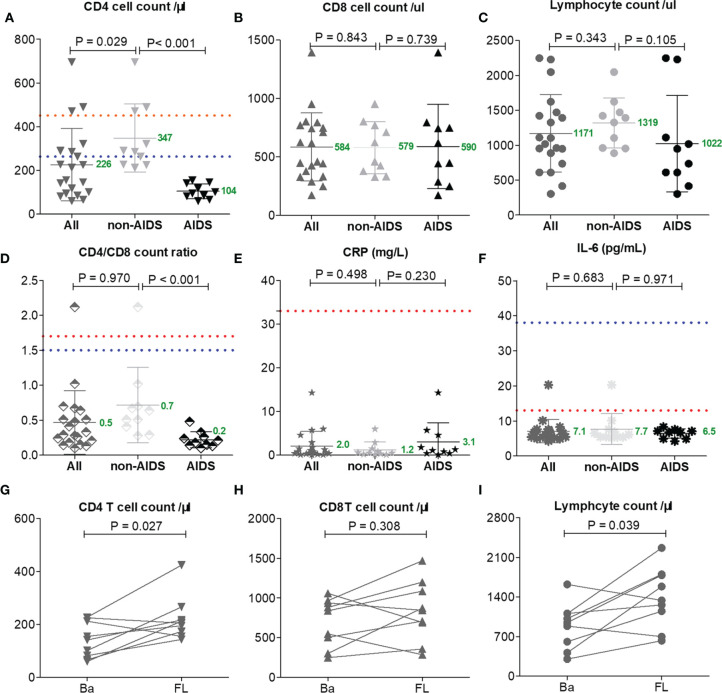
T-cell reduction is an important characteristic of coronavirus disease 2019 (COVID-19), and its immunopathology is a subject of debate. It may be due to the direct effect of the virus on T-cell exhaustion or indirectly due to T cells redistributing to the lungs. HIV/AIDS naturally served as a T-cell exhaustion disease model for recognizing how the immune system works in the course of COVID-19. In this study, we collected the clinical charts, T-lymphocyte analysis, and chest CT of HIV patients with laboratory-confirmed COVID-19 infection who were admitted to Jin Yin-tan Hospital (Wuhan, China). The median age of the 21 patients was 47 years [interquartile range (IQR) = 40-50 years] and the median CD4 T-cell count was 183 cells/μl (IQR = 96-289 cells/μl). Eleven HIV patients were in the non-AIDS stage and 10 were in the AIDS stage. Nine patients received antiretroviral treatment (ART) and 12 patients did not receive any treatment. Compared to the reported mortality rate (nearly 4%-10%) and severity rate (up to 20%-40%) among COVID-19 patients in hospital, a benign duration with 0% severity and mortality rates was shown by 21 HIV/AIDS patients. The severity rates of COVID-19 were comparable between non-AIDS (median CD4 = 287 cells/μl) and AIDS (median CD4 = 97 cells/μl) patients, despite some of the AIDS patients having baseline lung injury stimulated by HIV: 7 patients (33%) were mild (five in the non-AIDS group and two in the AIDS group) and 14 patients (67%) were moderate (six in the non-AIDS group and eight in the AIDS group). More importantly, we found that a reduction in T-cell number positively correlates with the serum levels of interleukin 6 (IL-6) and C-reactive protein (CRP), which is contrary to the reported findings on the immune response of COVID-19 patients (lower CD4 T-cell counts with higher levels of IL-6 and CRP). In HIV/AIDS, a compromised immune system with lower CD4 T-cell counts might waive the clinical symptoms and inflammatory responses, which suggests lymphocyte redistribution as an immunopathology leading to lymphopenia in COVID-19.
Keywords: COVID-19; HIV; T cells; T-cell exhaustion; lymphocyte redistribution.
Copyright © 2021 Lin, Lin, Wang, Wen, Xiang, Fan, Li, Wu, Lin, Lin, Sun, Chen, Chen, Lian, Xie, Lin, Xie, Li, Peng, Wang, Lin, Chen, Huang and Fu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinical and Immune Features of Hospitalized Pediatric Patients With Coronavirus Disease 2019 (COVID-19) in Wuhan, China.JAMA Netw Open. 2020 Jun 1;3(6):e2010895. doi: 10.1001/jamanetworkopen.2020.10895. JAMA Netw Open. 2020. PMID: 32492165 Free PMC article.
-
Thymosin Alpha-1 Has no Beneficial Effect on Restoring CD4+ and CD8+ T Lymphocyte Counts in COVID-19 Patients.Front Immunol. 2021 Jun 3;12:568789. doi: 10.3389/fimmu.2021.568789. eCollection 2021. Front Immunol. 2021. PMID: 34149679 Free PMC article.
-
Suppressed T cell-mediated immunity in patients with COVID-19: A clinical retrospective study in Wuhan, China.J Infect. 2020 Jul;81(1):e51-e60. doi: 10.1016/j.jinf.2020.04.012. Epub 2020 Apr 18. J Infect. 2020. PMID: 32315725 Free PMC article.
-
Association of Hospitalization Rate, Mortality, and CD4 T Cell Count with Comorbidity of COVID-19 and HIV: A Systematic Review and Meta-Analysis.AIDS Res Hum Retroviruses. 2023 Jul;39(7):332-339. doi: 10.1089/AID.2022.0076. Epub 2023 Apr 21. AIDS Res Hum Retroviruses. 2023. PMID: 36924275
-
Sharing CD4+ T Cell Loss: When COVID-19 and HIV Collide on Immune System.Front Immunol. 2020 Dec 15;11:596631. doi: 10.3389/fimmu.2020.596631. eCollection 2020. Front Immunol. 2020. PMID: 33384690 Free PMC article. Review.
Cited by
-
Ebselen and Diphenyl Diselenide Inhibit SARS-CoV-2 Replication at Non-Toxic Concentrations to Human Cell Lines.Vaccines (Basel). 2023 Jul 10;11(7):1222. doi: 10.3390/vaccines11071222. Vaccines (Basel). 2023. PMID: 37515038 Free PMC article.
-
SARS-CoV-2 Vaccine-Induced T-Cell Response after Three Doses in People Living with HIV on Antiretroviral Therapy Compared to Seronegative Controls (CTN 328 COVAXHIV Study).Viruses. 2023 Feb 19;15(2):575. doi: 10.3390/v15020575. Viruses. 2023. PMID: 36851789 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous