

Human viral encephalitis associated with suid herpesvirus 1
- PMID: 34647219
- PMCID: PMC8514202
- DOI: 10.1007/s10072-021-05633-0
Human viral encephalitis associated with suid herpesvirus 1
Abstract
Background: Suid herpesvirus type 1 (SHV1) is a type of neurotropic virus able to infect various species. However, the clinical cases of human SHV1 encephalitis are still rarely reported, and the clinical characteristics, treatment, and prognosis of human SHV1 encephalitis are still unclear.
Methods: In this study, we reported 2 cases of human encephalitis associated with SHV1 infection and reviewed the other 18 cases from the literatures. A total of 20 cases with human SHV1 encephalitis were summarized and re-analyzed.
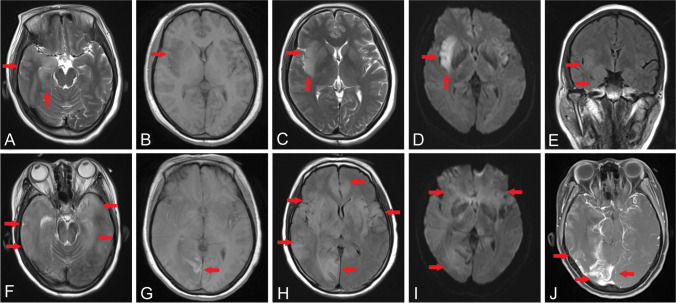
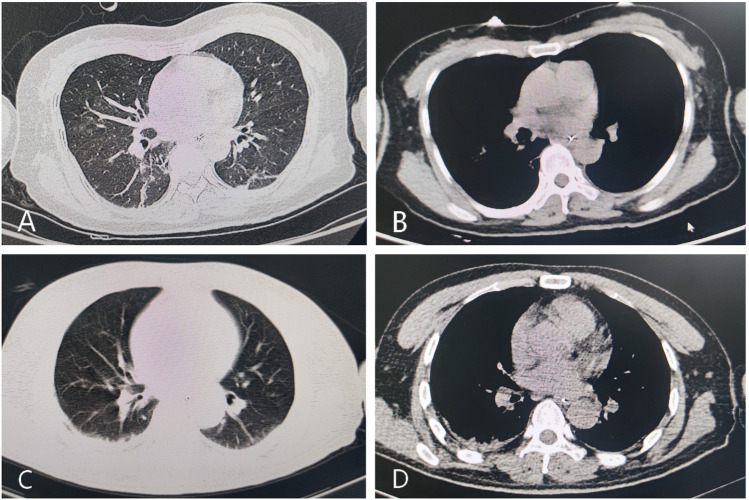
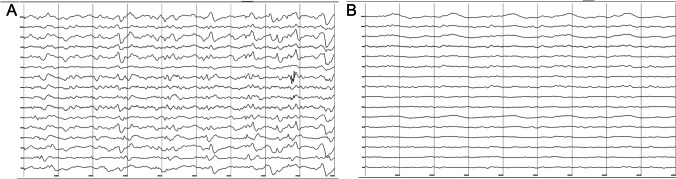
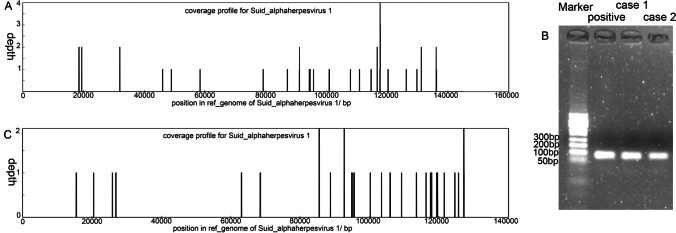
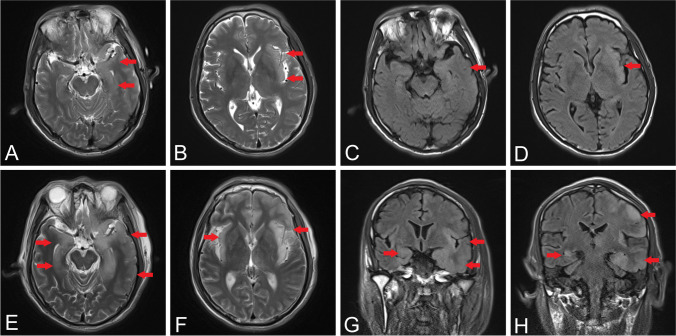
Results: Nineteen of 20 patients had a history of swine-related occupational exposure before illness onset. All patients initially presented with influenza-like symptoms and then developed seizures, disturbed consciousness, and endophthalmitis. All patients with clinical outcome of modified Rankin Scale of 5 or 6 suffered from rapid progressive respiratory failure. The results of cerebrospinal fluid (CSF) indicated aseptic or viral infection. MRI findings of SHV1 encephalitis were prone to distribute in temporal-frontal and insular cortex, which was similar to the pattern of herpes simplex virus encephalitis, while some cases with involvements of gray matter nuclei had a high rate of mortality. Metagenomic next-generation sequencing (mNGS) revealed that all patients had unique SHV1 sequences with variable reads in the CSF.
Conclusions: The variant SHV1 can cause a new type of human viral encephalitis, characterized by acute, fulminating, and catastrophic central nervous system infection. Rapid progressive respiratory failure and extensive lesions of deep gray matter nuclei might be indicators to poor prognosis. No approved treatments for the encephalitis are available, but it is possible to diagnose encephalitis quickly by mNGS.
Keywords: Suid herpesvirus type 1; Pseudorabies virus; Encephalitis; Metagenomic next-generation sequencing.
© 2021. Fondazione Società Italiana di Neurologia.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Human encephalitis caused by pseudorabies virus infection: a case report.J Neurovirol. 2020 Jun;26(3):442-448. doi: 10.1007/s13365-019-00822-2. Epub 2020 Jan 2. J Neurovirol. 2020. PMID: 31898060 Free PMC article.
-
[Value of the polymerase chain reaction in the diagnosis of herpes infections of the nervous system].Enferm Infecc Microbiol Clin. 2004 Mar;22(3):150-5. doi: 10.1016/s0213-005x(04)73055-4. Enferm Infecc Microbiol Clin. 2004. PMID: 14987535 Spanish.
-
A Novel Human Acute Encephalitis Caused by Pseudorabies Virus Variant Strain.Clin Infect Dis. 2021 Dec 6;73(11):e3690-e3700. doi: 10.1093/cid/ciaa987. Clin Infect Dis. 2021. PMID: 32667972
-
Human Encephalitis Caused by Pseudorabies Virus in China: A Case Report and Systematic Review.Vector Borne Zoonotic Dis. 2022 Jul;22(7):391-396. doi: 10.1089/vbz.2022.0002. Epub 2022 Jun 23. Vector Borne Zoonotic Dis. 2022. PMID: 35736787
-
From Severe Herpes Zoster to Rare Suid Herpesvirus Encephalitis: A New Twist of the Varicellovirus Genus Infection in Patients with Kidney Diseases.Int J Med Sci. 2020 Mar 5;17(6):745-750. doi: 10.7150/ijms.41952. eCollection 2020. Int J Med Sci. 2020. PMID: 32218696 Free PMC article. Review.
Cited by
-
Membrane fusion, potential threats, and natural antiviral drugs of pseudorabies virus.Vet Res. 2023 May 2;54(1):39. doi: 10.1186/s13567-023-01171-z. Vet Res. 2023. PMID: 37131259 Free PMC article. Review.
-
The Role of Latency-Associated Transcripts in the Latent Infection of Pseudorabies Virus.Viruses. 2022 Jun 24;14(7):1379. doi: 10.3390/v14071379. Viruses. 2022. PMID: 35891360 Free PMC article. Review.
-
The Epidemiology and Variation in Pseudorabies Virus: A Continuing Challenge to Pigs and Humans.Viruses. 2022 Jul 1;14(7):1463. doi: 10.3390/v14071463. Viruses. 2022. PMID: 35891443 Free PMC article. Review.
-
Infectivity and Potential Zoonotic Characteristics of Porcine Pseudorabies Virus in Human Cells.Transbound Emerg Dis. 2024 Jul 16;2024:5929976. doi: 10.1155/2024/5929976. eCollection 2024. Transbound Emerg Dis. 2024. PMID: 40303056 Free PMC article.
-
Viral Metagenomics for the Identification of Emerging Infections in Clinical Samples with Inconclusive Dengue, Zika, and Chikungunya Viral Amplification.Viruses. 2022 Aug 31;14(9):1933. doi: 10.3390/v14091933. Viruses. 2022. PMID: 36146740 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
