

Lipoprotein(a): A Genetically Determined, Causal, and Prevalent Risk Factor for Atherosclerotic Cardiovascular Disease: A Scientific Statement From the American Heart Association
- PMID: 34647487
- PMCID: PMC9989949
- DOI: 10.1161/ATV.0000000000000147
Lipoprotein(a): A Genetically Determined, Causal, and Prevalent Risk Factor for Atherosclerotic Cardiovascular Disease: A Scientific Statement From the American Heart Association
Abstract
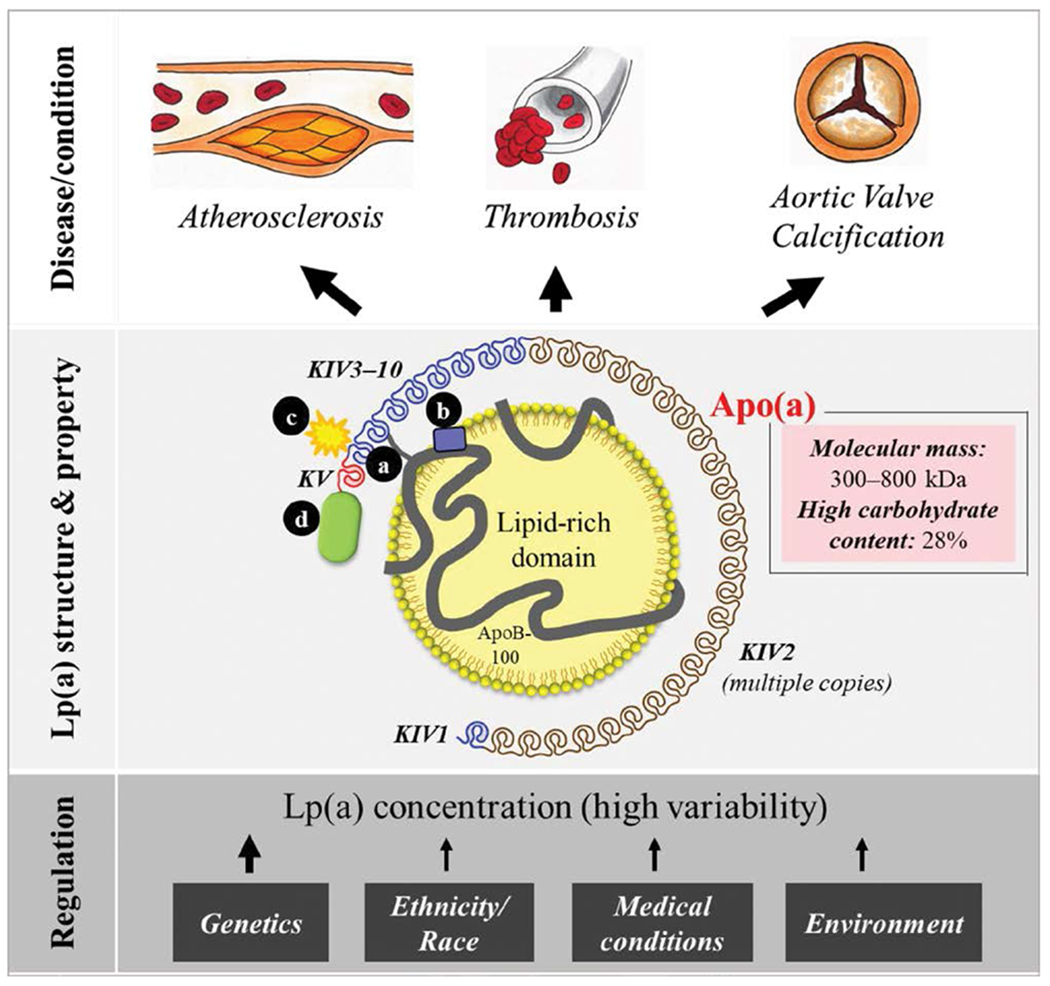
High levels of lipoprotein(a) [Lp(a)], an apoB100-containing lipoprotein, are an independent and causal risk factor for atherosclerotic cardiovascular diseases through mechanisms associated with increased atherogenesis, inflammation, and thrombosis. Lp(a) is predominantly a monogenic cardiovascular risk determinant, with ≈70% to ≥90% of interindividual heterogeneity in levels being genetically determined. The 2 major protein components of Lp(a) particles are apoB100 and apolipoprotein(a). Lp(a) remains a risk factor for cardiovascular disease development even in the setting of effective reduction of plasma low-density lipoprotein cholesterol and apoB100. Despite its demonstrated contribution to atherosclerotic cardiovascular disease burden, we presently lack standardization and harmonization of assays, universal guidelines for diagnosing and providing risk assessment, and targeted treatments to lower Lp(a). There is a clinical need to understand the genetic and biological basis for variation in Lp(a) levels and its relationship to disease in different ancestry groups. This scientific statement capitalizes on the expertise of a diverse basic science and clinical workgroup to highlight the history, biology, pathophysiology, and emerging clinical evidence in the Lp(a) field. Herein, we address key knowledge gaps and future directions required to mitigate the atherosclerotic cardiovascular disease risk attributable to elevated Lp(a) levels.
Keywords: AHA Scientific Statements; apolipoprotein B100; atherosclerotic cardiovascular disease; cholesterol, low-density lipoprotein; lipoprotein(a).
Conflict of interest statement
The American Heart Association makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
Figures
References
-
- Xu J, Murphy SL, Kockanek KD, Arias E. Mortality in the United States, 2018. NCHS Data Brief. 2020;355:1–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
