

Contribution of Alzheimer's biomarkers and risk factors to cognitive impairment and decline across the Alzheimer's disease continuum
- PMID: 34647694
- PMCID: PMC9014819
- DOI: 10.1002/alz.12480
Contribution of Alzheimer's biomarkers and risk factors to cognitive impairment and decline across the Alzheimer's disease continuum
Abstract
Introduction: Amyloid beta (Aβ), tau, and neurodegeneration jointly with the Alzheimer's disease (AD) risk factors affect the severity of clinical symptoms and disease progression.
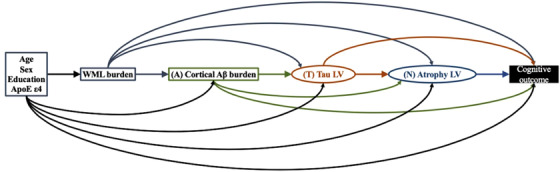
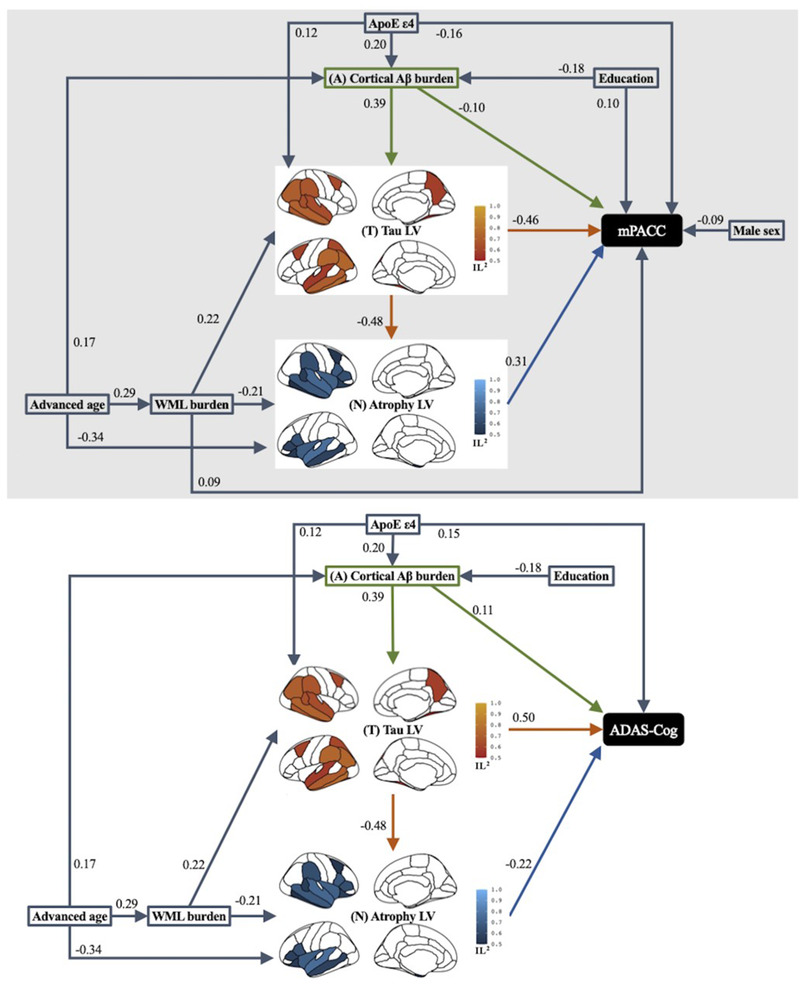
Methods: Within 248 Aβ-positive elderly with and without cognitive impairment and dementia, partial least squares structural equation pathway modeling was used to assess the direct and indirect effects of imaging biomarkers (global Aβ-positron emission tomography [PET] uptake, regional tau-PET uptake, and regional magnetic resonance imaging-based atrophy) and risk-factors (age, sex, education, apolipoprotein E [APOE], and white-matter lesions) on cross-sectional cognitive impairment and longitudinal cognitive decline.
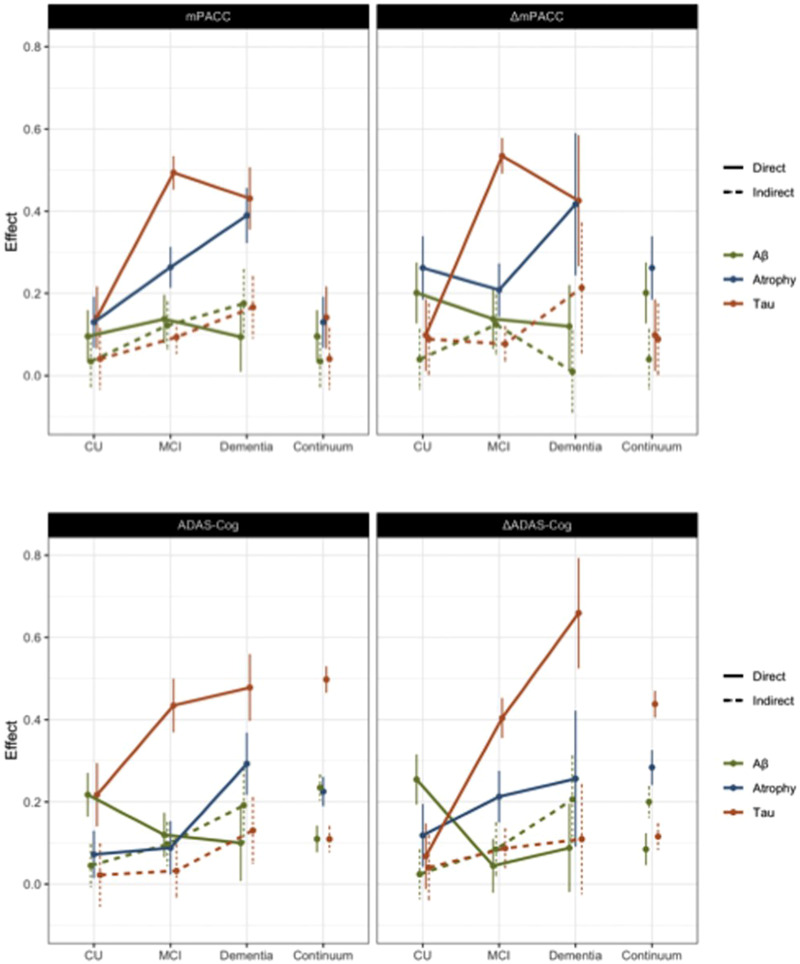
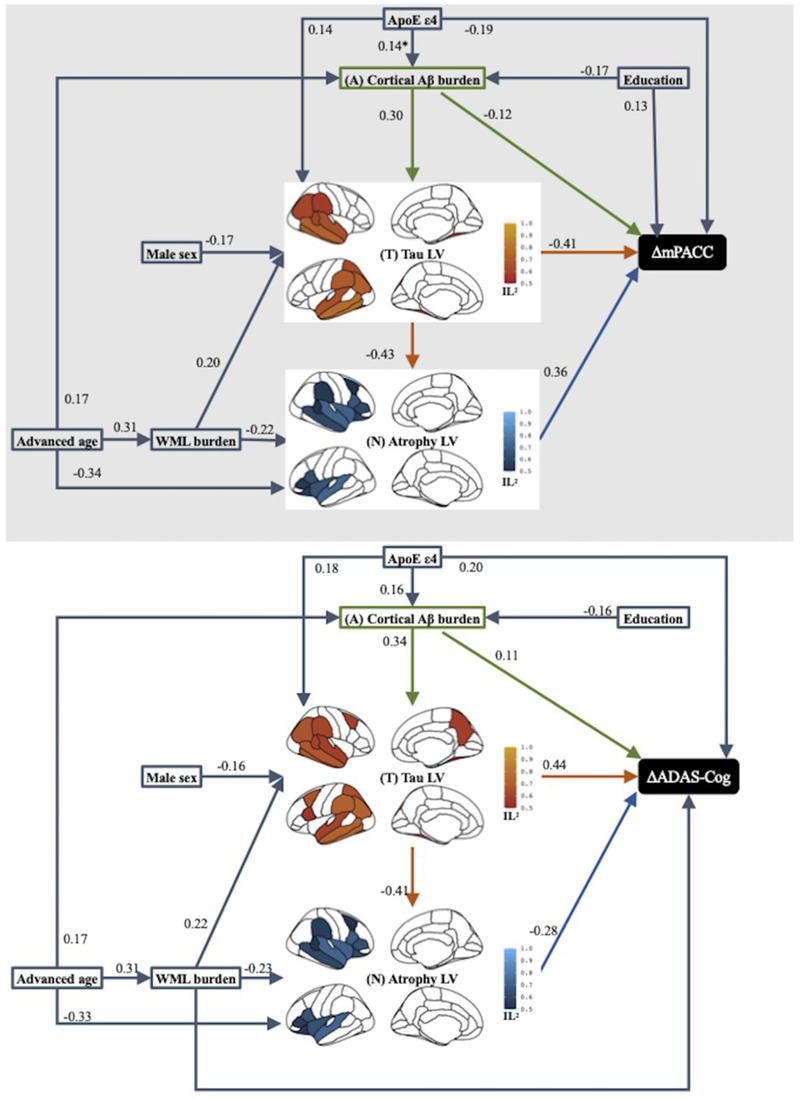
Results: Sixteen percent of variance in cross-sectional cognitive impairment was accounted for by Aβ, 46% to 47% by tau, and 25% to 29% by atrophy, although 53% to 58% of total variance in cognitive impairment was explained by incorporating mediated and direct effects of AD risk factors. The Aβ-tau-atrophy pathway accounted for 50% to 56% of variance in longitudinal cognitive decline while Aβ, tau, and atrophy independently explained 16%, 46% to 47%, and 25% to 29% of the variance, respectively.
Discussion: These findings emphasize that treatments that remove Aβ and completely stop downstream effects on tau and neurodegeneration would only be partially effective in slowing of cognitive decline or reversing cognitive impairment.
Keywords: Alzheimer's Disease Assessment Scale-Cognitive Subscale; Preclinical Alzheimer Cognitive Composite; amyloid beta; atrophy; cognition; magnetic resonance imaging; positron emission tomography; tau; white matter lesions.
© 2021 The Authors. Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
Dr. Weintraub reports grants from NIA, Department of Veterans Affairs, Fox Foundation, Acadia Pharmaceuticals, and IPMDS. All payments made to U. Pennsylvania, compensation for licensing of QUIP, QUIP‐RS, and PDAQ‐15 through the University of Pennsylvania. He received personal consulting compensation from Acadia, Aptinyx, CHDI Foundation, Clintrex LLC (Otsuka), Eisai, Great Lake Neurotechnologies, Janssen, Sage, Scion, Signant Health, Sunovion, and Vanda. He serves as Chair DSMB for ATRI and ADCS. Dr. Aisen has received support over the last 36 months from payments to his institution from NIA, FNIH, Alzheimer's Association, Janssen, Lilly, Merck, and Eisai. He has served on the advisory boards of Biogen, Merck, Roche, Abbvie, Rainbow Medical, ImmunoBrain Checkpoint, Shionogi, and has no other support or conflicts of interest to declare. Dr. Jack was supported in the current work by NIH funding. Over the last 36 months, he has received support from NIH grants and the Alexander Family Alzheimer's Disease Research Professorship of the Mayo Clinic to his institution and has served on the advisory boards of iDMC and Roche with no payments made. He serves on an independent data monitoring board for Roche, has consulted for and served as a speaker for Eisai, and consulted for Biogen, but he receives no personal compensation from any commercial entity. He has no other support or conflicts of interest to declare. Dr. Jagust has received support over the last 36 months from grants to his institution (NIH grants R01 AG034570 [Dr. Jagust], R01AG062542 [Dr. Jagust], U24 AG067418 [Dr. Jagust], P01AG019724 [Dr. Bruce Miller], R01 AG031164 [Dr. Matthew Walker], RF1 AG054019 [Dr. Matthew Walker], U01 AG024904 [Dr. Weiner], RF1 AG054106‐01A1 [Dr. Matthew Walker], R44AG046025‐03 [Dr. Daojing Wang], R01 AG061303 [Dr. Lexin Li], MH112775 [Dr. Ming Hsu], 1R01AG062689‐01 [Dr. Landau], AG062624 [Dr. José Luchsinger], and R01AG069090), direct consulting fees (Biogen, Bioclinica, Genentech/Roche, CuraSen, Grifols), and has served on the advisory board of the Alzheimer's Prevention Initiative. He has no other support or conflicts of interest to declare. Dr. Petersen over the past 36 months received grants through his institution (P30 AG062677, U01 AG006786); licenses or royalties from Oxford University Press and UpToDate; and consulting fees from Roche, Merck, Biogen, Genentech, and Eisai. He served on the advisory board of Genentech and has no other support or conflicts of interest to declare. Dr. Saykin was supported in this work by grants from NIH and Department of Defense (NIH grants U01 AG024904, P30 AG010133, R01 AG019771, R01 LM013463, R01 LM011360 and DoD grants W81XWH‐13‐1‐0259 and W81XWH‐12‐2‐0012), and over the past 36 months received support from grants to his institution (as detailed above). He served on the Bayer Oncology Advisory Board and received PET tracer precursor from Eli Lilly/Avid Radiopharmaceuticals. He reports personal fees from Arkley BioTek and Springer Nature, outside the submitted work. He has no other support or conflicts of interest to declare. Dr. Shaw has received over the past 36 months grants through his institution (NIH grants U01 AG024904 (ADNI3), UPenn ADRC NIA grant for Biomarker Core; Michael J. Fox Foundation for Parkinson's Research for AD biomarker studies; Roche IIS for AD biomarker studies), fees for the Biogen Teaching program on AD Biomarkers, and travel funds from NIA ADNI3 Biomarker Core. He has served on the Roche Advisory Board, LEADS Advisory Board, and Fujirebio Advisory Board. He received in kind support from Roche (immunoassay reagents and equipment) for ADNI3. He has no other support or conflicts of interest to declare. Dr. Trojanowski has received over the past 36 months grants through his institution (AG10124). He has no other support or conflicts of interest to declare. Dr. Weiner is the Principal Investigator of NIH funded grants. Over the past 36 months he received funding administered through his institutions (NIH grants: 1RF1AG059009‐01 and 1R01AG058676‐01A1; CA Dept. of Health grant: 19‐10616; NIH Subaward from Dr. Richard Gershon: 1U2CA060426‐01), consulting fees (Cerecin/Accera, Inc., BioClinica, Nestle/Nestec, Roche, Genentech, NIH, The Buck Institute for Research on Aging, FUJIFILM‐Toyama Chemical [Japan], Garfield Weston, Baird Equity Capital, University of Southern California [USC], Cytox, and Japanese Organization for Medical Device Development, Inc. [JOMDD] and T3D Therapeutics), and payment for lecturing (The Buck Institute for Research on Aging). He holds stock options in Anven, Alzheon, and Aleca. He receives other grant support for his work (NIH: 5U19AG024904‐14; 1R01AG053798‐01A1; R01 MH098062; U24 AG057437‐01; 1U2CA060426‐01; 1R01AG058676‐01A1; and 1RF1AG059009‐01, DOD: W81XWH‐15‐2‐0070; 0W81XWH‐12‐2‐0012; W81XWH‐14‐1‐0462; W81XWH‐13‐1‐0259, PCORI: PPRN‐1501‐26817, California Dept. of Public Health: 16‐10054, U. Michigan: 18‐PAF01312, Siemens: 444951‐54249, Biogen: 174552, Hillblom Foundation: 2015‐A‐011‐NET, Alzheimer's Association: BHR‐16‐459161; The State of California: 18‐109929). He also receives support from Johnson & Johnson, Kevin and Connie Shanahan, GE, VUmc, Australian Catholic University (HBI‐BHR), The Stroke Foundation, and the Veterans Administration. He has served on advisory boards for Eli Lilly, Cerecin/Accera, Roche, Alzheon, Inc., Merck Sharp & Dohme Corp., Nestle/Nestec, PCORI/PPRN, Dolby Family Ventures, National Institute on Aging (NIA), Brain Health Registry, and ADNI. He has no other support or conflicts of interest to declare.
Figures
References
-
- Budd Haeberlein S, O'Gorman J, Chiao P, et al. Clinical development of aducanumab, an anti‐aβ human monoclonal antibody being investigated for the treatment of early Alzheimer's disease. J Prev Alzheimers Dis. 2017;4:255‐263. - PubMed
-
- Honig LS, Vellas B, Woodward M, et al. Trial of solanezumab for mild dementia due to Alzheimer's disease. N Engl J Med. 2018;378:321‐330. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
