

Linear concentration-response relationship of serum caffeine with adenosine-induced fractional flow reserve overestimation: a comparison with papaverine
- PMID: 34647891
- PMCID: PMC9725067
- DOI: 10.4244/EIJ-D-21-00453
Linear concentration-response relationship of serum caffeine with adenosine-induced fractional flow reserve overestimation: a comparison with papaverine
Abstract
Background: Caffeine intake from one cup of coffee one hour before adenosine stress tests, corresponding to serum caffeine levels of 3-4 mg/L, is thought to be acceptable for non-invasive imaging.
Aims: We aimed to elucidate whether serum caffeine is independently associated with adenosine-induced fractional flow reserve (FFR) overestimation and their concentration-response relationship.
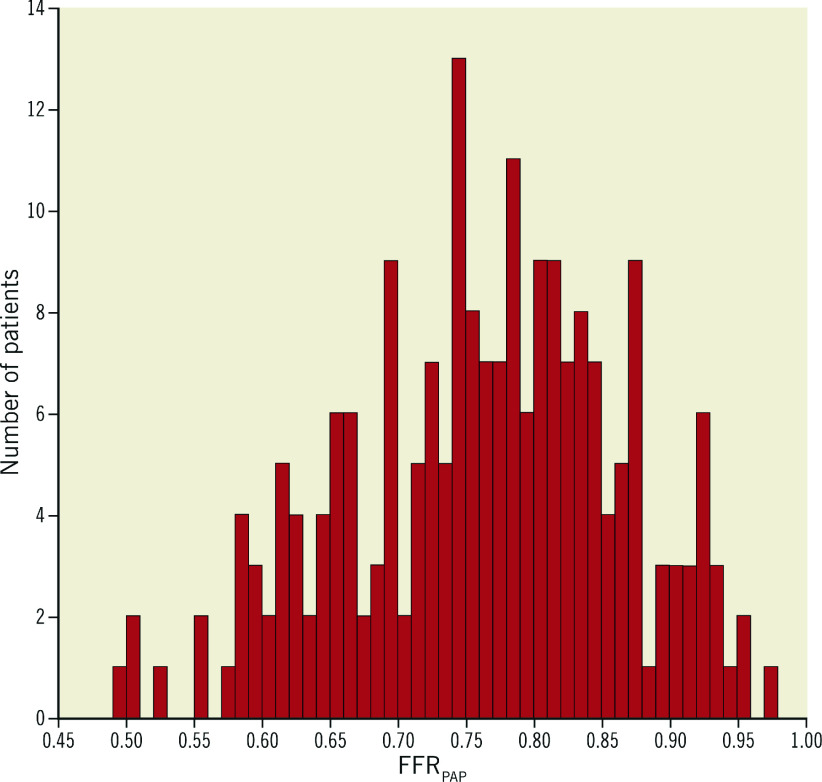
Methods: FFR was measured using adenosine (FFRADN) and papaverine (FFRPAP) in 209 patients. FFRADN overestimation was defined as FFRADN - FFRPAP. The locally weighted scatterplot smoothing (LOWESS) approach was applied to evaluate the relationship between serum caffeine level and FFRADN overestimation. Multiple regression analysis was used to determine independent factors associated with FFRADN overestimation.
Results: Caffeine was ingested at <12 hours in 85 patients, at 12-24 hours in 35 patients, and at >24 hours in 89 patients. Multiple regression analysis identified serum caffeine level as the strongest factor associated with FFRADN overestimation (p<0.001). The LOWESS curve demonstrated that FFRADN overestimation started from just above the lower detection limit of serum caffeine and increased approximately 0.01 FFR unit per 1 mg/L increase in serum caffeine level with a linear relationship. The 90th percentile of serum caffeine levels for the ≤12-hour, the 12-24-hour, and the >24-hour groups corresponded to FFRADN overestimations by 0.06, 0.03, and 0.02, respectively.
Conclusions: Serum caffeine overestimates FFRADN values in a linear concentration-response manner. FFRADN overestimation occurs at much lower serum caffeine levels than those that were previously believed. Our results highlight that standardised caffeine control is required for reliable adenosine-induced FFR measurements.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures


Comment in
-
Letter: Caffeine and fractional flow reserve overestimation: a word of caution.EuroIntervention. 2022 Aug 19;18(6):524. doi: 10.4244/EIJ-D-21-01009L. EuroIntervention. 2022. PMID: 35983739 Free PMC article. No abstract available.
References
-
- Fihn SD, Blankenship JC, Alexander KP, Bittl JA, Byrne JG, Fletcher BJ, Fonarow GC, Lange RA, Levine GN, Maddox TM, Naidu SS, Ohman EM, Smith PK. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2014;64:1929–49. doi: 10.1016/j.jacc.2014.07.017. - DOI - PubMed
-
- Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, Byrne RA, Collet JP, Falk V, Head SJ, Jüni P, Kastrati A, Koller A, Kristensen SD, Niebauer J, Richter DJ, Seferovic PM, Sibbing D, Stefanini GG, Windecker S, Yadav R, Zembala MO ESC Scientific Document Group. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40:87–165. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources