

Predictability of Mortality in Patients With Myocardial Injury After Noncardiac Surgery Based on Perioperative Factors via Machine Learning: Retrospective Study
- PMID: 34647900
- PMCID: PMC8554678
- DOI: 10.2196/32771
Predictability of Mortality in Patients With Myocardial Injury After Noncardiac Surgery Based on Perioperative Factors via Machine Learning: Retrospective Study
Abstract
Background: Myocardial injury after noncardiac surgery (MINS) is associated with increased postoperative mortality, but the relevant perioperative factors that contribute to the mortality of patients with MINS have not been fully evaluated.
Objective: To establish a comprehensive body of knowledge relating to patients with MINS, we researched the best performing predictive model based on machine learning algorithms.
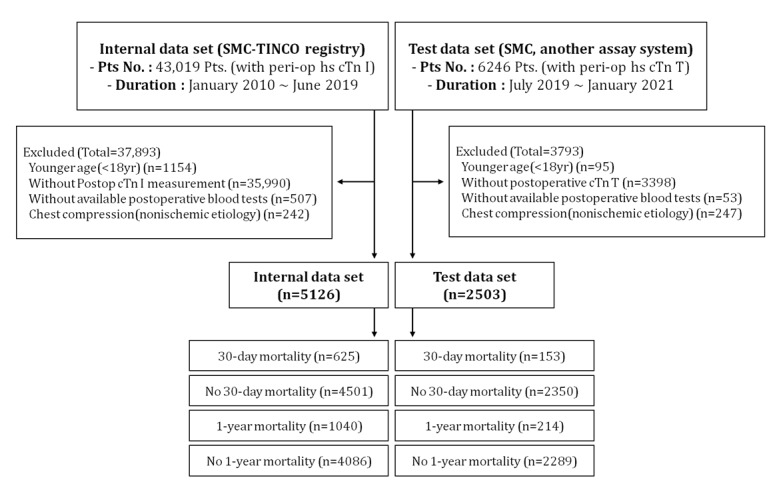
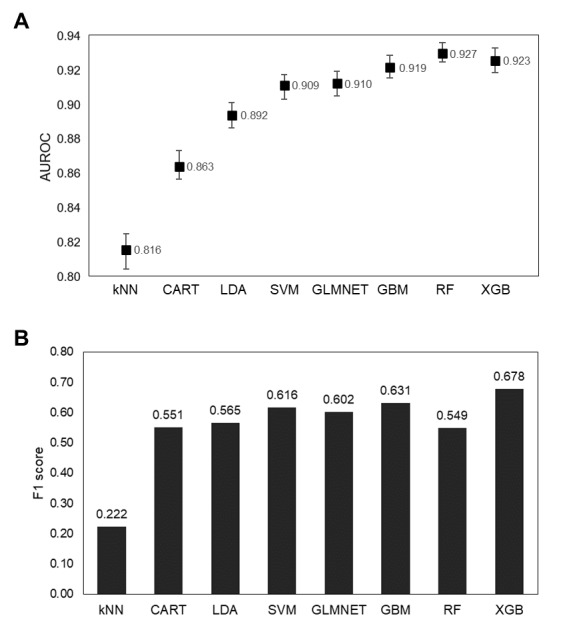
Methods: Using clinical data from 7629 patients with MINS from the clinical data warehouse, we evaluated 8 machine learning algorithms for accuracy, precision, recall, F1 score, area under the receiver operating characteristic (AUROC) curve, and area under the precision-recall curve to investigate the best model for predicting mortality. Feature importance and Shapley Additive Explanations values were analyzed to explain the role of each clinical factor in patients with MINS.
Results: Extreme gradient boosting outperformed the other models. The model showed an AUROC of 0.923 (95% CI 0.916-0.930). The AUROC of the model did not decrease in the test data set (0.894, 95% CI 0.86-0.922; P=.06). Antiplatelet drugs prescription, elevated C-reactive protein level, and beta blocker prescription were associated with reduced 30-day mortality.
Conclusions: Predicting the mortality of patients with MINS was shown to be feasible using machine learning. By analyzing the impact of predictors, markers that should be cautiously monitored by clinicians may be identified.
Keywords: extreme gradient boosting; high-sensitivity cardiac troponin; machine learning; myocardial injury after noncardiac surgery.
©Seo Jeong Shin, Jungchan Park, Seung-Hwa Lee, Kwangmo Yang, Rae Woong Park. Originally published in JMIR Medical Informatics (https://medinform.jmir.org), 14.10.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures


References
-
- Puelacher C, Lurati Buse G, Seeberger D, Sazgary L, Marbot S, Lampart A, Espinola J, Kindler C, Hammerer A, Seeberger E, Strebel I, Wildi K, Twerenbold R, du Fay de Lavallaz J, Steiner L, Gurke L, Breidthardt T, Rentsch K, Buser A, Gualandro DM, Osswald S, Mueller C, BASEL-PMI Investigators Perioperative myocardial injury after noncardiac surgery: incidence, mortality, and characterization. Circulation. 2018 Mar 20;137(12):1221–1232. doi: 10.1161/CIRCULATIONAHA.117.030114.CIRCULATIONAHA.117.030114 - DOI - PubMed
-
- Smilowitz NR, Redel-Traub G, Hausvater A, Armanious A, Nicholson J, Puelacher C, Berger JS. Myocardial injury after noncardiac surgery: a systematic review and meta-analysis. Cardiol Rev. 2019;27(6):267–273. doi: 10.1097/CRD.0000000000000254. http://europepmc.org/abstract/MED/30985328 - DOI - PMC - PubMed
-
- van Waes JAR, van Klei WA, Wijeysundera DN, van Wolfswinkel L, Lindsay TF, Beattie WS. Association between intraoperative hypotension and myocardial injury after vascular surgery. Anesthesiology. 2016 Jan;124(1):35–44. doi: 10.1097/ALN.0000000000000922. https://pubs.asahq.org/anesthesiology/article-lookup/doi/10.1097/ALN.000... - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
