

Effect of Intraoperative Dexmedetomidine on Recovery of Gastrointestinal Function After Abdominal Surgery in Older Adults: A Randomized Clinical Trial
- PMID: 34648009
- PMCID: PMC8517746
- DOI: 10.1001/jamanetworkopen.2021.28886
Effect of Intraoperative Dexmedetomidine on Recovery of Gastrointestinal Function After Abdominal Surgery in Older Adults: A Randomized Clinical Trial
Abstract
Importance: Postoperative ileus is common after abdominal surgery, and small clinical studies have reported that intraoperative administration of dexmedetomidine may be associated with improvements in postoperative gastrointestinal function. However, findings have been inconsistent and study samples have been small. Further examination of the effects of intraoperative dexmedetomidine on postoperative gastrointestinal function is needed.
Objective: To evaluate the effects of intraoperative intravenous dexmedetomidine vs placebo on postoperative gastrointestinal function among older patients undergoing abdominal surgery.
Design, setting, and participants: This multicenter, double-blind, placebo-controlled randomized clinical trial was conducted at the First Affiliated Hospital of Anhui Medical University in Hefei, China (lead site), and 12 other tertiary hospitals in Anhui Province, China. A total of 808 participants aged 60 years or older who were scheduled to receive abdominal surgery with an expected surgical duration of 1 to 6 hours were enrolled. The study was conducted from August 21, 2018, to December 9, 2019.
Interventions: Dexmedetomidine infusion (a loading dose of 0.5 μg/kg over 15 minutes followed by a maintenance dose of 0.2 μg/kg per hour) or placebo infusion (normal saline) during surgery.
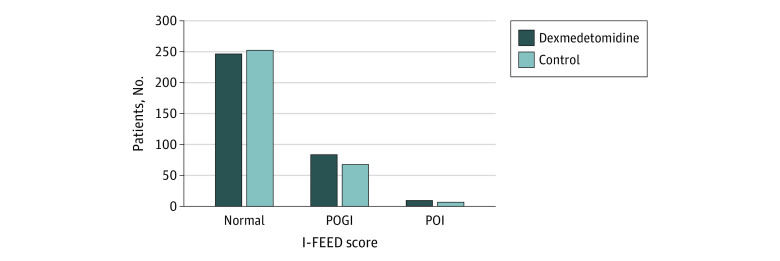
Main outcomes and measures: The primary outcome was time to first flatus. Secondary outcomes were postoperative gastrointestinal function measured by the I-FEED (intake, feeling nauseated, emesis, physical examination, and duration of symptoms) scoring system, time to first feces, time to first oral feeding, incidence of delirium, pain scores, sleep quality, postoperative nausea and vomiting, hospital costs, and hospital length of stay.
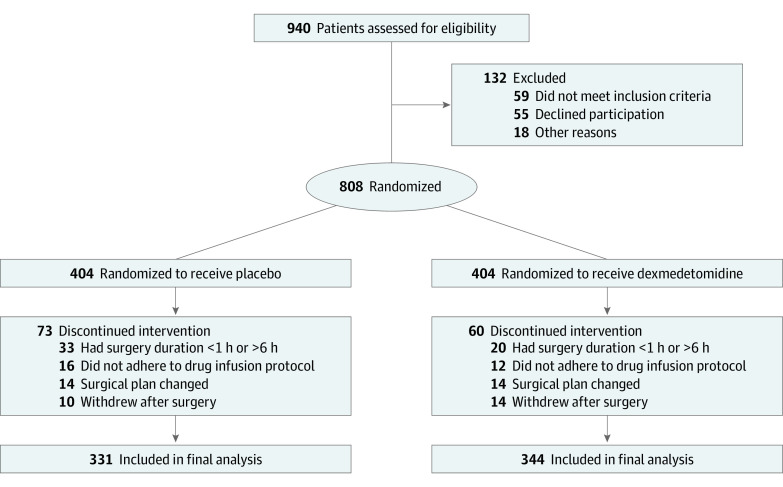
Results: Among 808 patients enrolled, 404 were randomized to receive intraoperative dexmedetomidine, and 404 were randomized to receive placebo. In total, 133 patients (60 in the dexmedetomidine group and 73 in the placebo group) were excluded because of protocol deviations, and 675 patients (344 in the dexmedetomidine group and 331 in the placebo group; mean [SD] age, 70.2 [6.1] years; 445 men [65.9%]) were included in the per-protocol analysis. The dexmedetomidine group had a significantly shorter time to first flatus (median, 65 hours [IQR, 48-78 hours] vs 78 hours [62-93 hours], respectively; P < .001), time to first feces (median, 85 hours [IQR, 68-115 hours] vs 98 hours [IQR, 74-121 hours]; P = .001), and hospital length of stay (median, 13 days [IQR, 10-17 days] vs 15 days [IQR, 11-18 days]; P = .005) than the control group. Postoperative gastrointestinal function (as measured by the I-FEED score) and delirium incidence were similar in the dexmedetomidine and control groups (eg, 248 patients [72.1%] vs 254 patients [76.7%], respectively, had I-FEED scores indicating normal postoperative gastrointestinal function; 18 patients [5.2%] vs 12 patients [3.6%] had delirium on postoperative day 3).
Conclusions and relevance: In this randomized clinical trial, the administration of intraoperative dexmedetomidine reduced the time to first flatus, time to first feces, and length of stay after abdominal surgery. These results suggest that this therapy may be a viable strategy to enhance postoperative recovery of gastrointestinal function among older adults.
Trial registration: Chinese Clinical Trial Registry Identifier: ChiCTR1800017232.
Conflict of interest statement
Figures
References
-
- Hedrick TL, McEvoy MD, Mythen MMG, et al. ; Perioperative Quality Initiative (POQI) 2 Workgroup . American Society for Enhanced Recovery and Perioperative Quality Initiative joint consensus statement on postoperative gastrointestinal dysfunction within an enhanced recovery pathway for elective colorectal surgery. Anesth Analg. 2018;126(6):1896-1907. doi:10.1213/ANE.0000000000002742 - DOI - PubMed
