

Interpretation of Abnormal Dexamethasone Suppression Test is Enhanced With Use of Synchronous Free Cortisol Assessment
- PMID: 34648626
- PMCID: PMC9006975
- DOI: 10.1210/clinem/dgab724
Interpretation of Abnormal Dexamethasone Suppression Test is Enhanced With Use of Synchronous Free Cortisol Assessment
Abstract
Context: Interpretation of dexamethasone suppression test (DST) may be influenced by dexamethasone absorption and metabolism and by the altered cortisol binding.
Objective: We aimed to determine the normal ranges of free cortisol during DST in participants without adrenal disorders and to identify the population of patients where post-DST free cortisol measurements add value to the diagnostic workup.
Design and setting: Cross-sectional study conducted in a tertiary medical center.
Participants: Adult volunteers without adrenal disorders (n = 168; 47 women on oral contraceptive therapy [OCP], 66 women not on OCP, 55 men) and patients undergoing evaluation for hypercortisolism (n = 196; 16 women on OCP).
Measurements: Post-DST dexamethasone and free cortisol (mass spectrometry) and total cortisol (immunoassay).
Main outcome measures: Reference range for post-DST free cortisol, diagnostic accuracy of post-DST total cortisol.
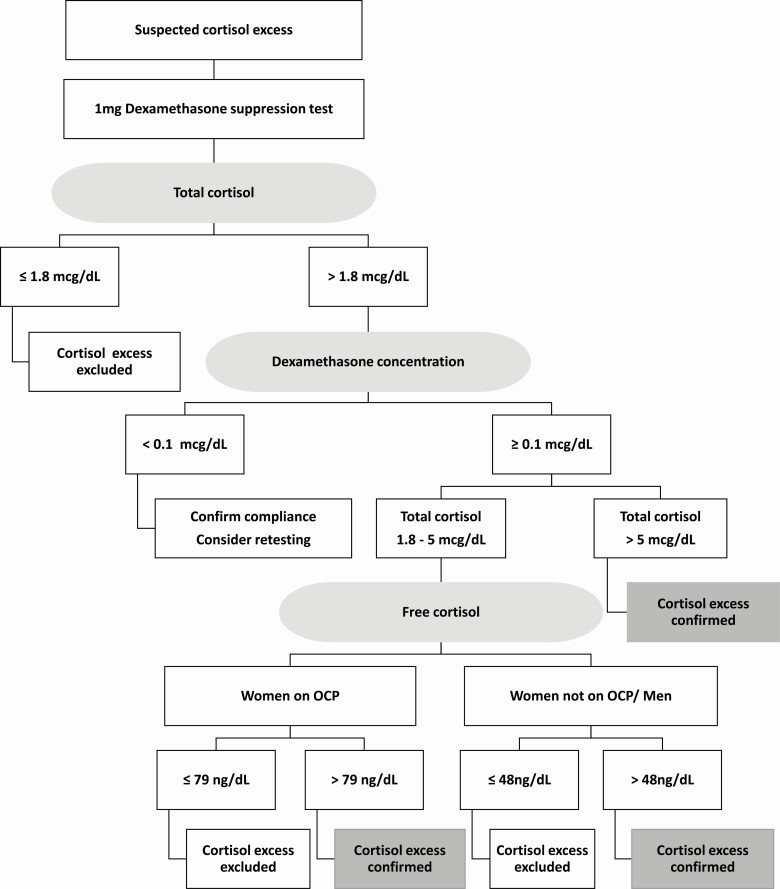
Results: Adequate dexamethasone concentrations (≥0.1 mcg/dL) were seen in 97.6% volunteers and 96.3% patients. Only 25.5% of women volunteers on OCP had abnormal post-DST total cortisol (>1.8 mcg/dL). In volunteers, the upper post-DST free cortisol range was 48 ng/dL in men and women not on OCP, and 79 ng/dL in women on OCP. When compared with post-DST free cortisol, diagnostic accuracy of post-DST total cortisol was 87.3% (95% CI, 81.7-91.7); all false-positive results occurred in patients with post-DST cortisol between 1.8 and 5 mcg/dL. OCP use was the only factor associated with false-positive results (21.1% vs 4.9%, P = 0.02).
Conclusions: Post-DST free cortisol measurements are valuable in patients with optimal dexamethasone concentrations and post-DST total cortisol between 1.8 and 5 mcg/dL.
Keywords: accuracy; adrenal adenoma; adrenal mass; diagnosis; mild autonomous cortisol secretion.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures


References
-
- Vaidya A, Hamrahian A, Bancos I, Fleseriu M, Ghayee HK. The evaluation of incidentally discovered adrenal masses. Endocr Pract. 2019;25(2):178-192. - PubMed
-
- Fassnacht M, Arlt W, Bancos I, et al. Management of adrenal incidentalomas: European Society of Endocrinology clinical practice guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2016;175(2):G1-G34. - PubMed
-
- Elhassan YS, Alahdab F, Prete A, et al. Natural history of adrenal incidentalomas with and without mild autonomous cortisol excess: a systematic review and meta-analysis. Ann Intern Med. 2019;171(2):107-116. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
