

A poor and delayed anti-SARS-CoV2 IgG response is associated to severe COVID-19 in children
- PMID: 34649078
- PMCID: PMC8502533
- DOI: 10.1016/j.ebiom.2021.103615
A poor and delayed anti-SARS-CoV2 IgG response is associated to severe COVID-19 in children
Abstract
Background: Most children and youth develop mild or asymptomatic disease during severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. However, a very small number of patients suffer severe Coronavirus induced disease 2019 (COVID-19). The reasons underlying these different outcomes remain unknown.
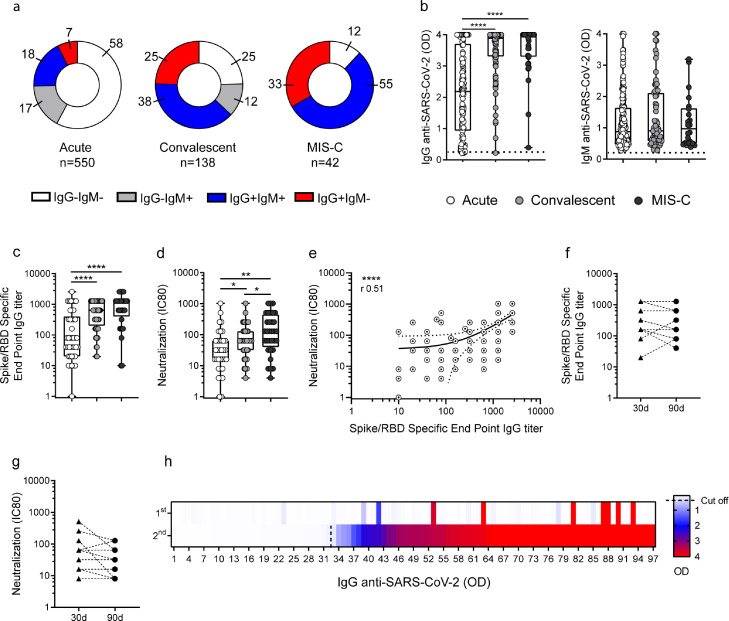
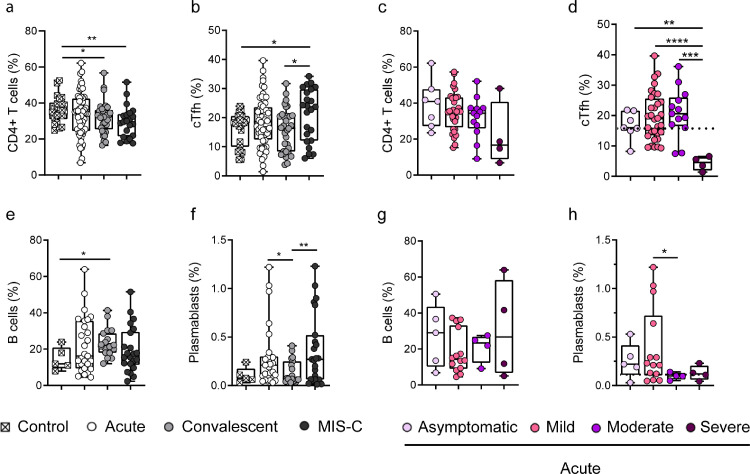
Methods: We analyzed three different cohorts: children with acute infection (n=550), convalescent children (n=138), and MIS-C (multisystem inflammatory syndrome in children, n=42). IgG and IgM antibodies to the spike protein of SARS-CoV-2, serum-neutralizing activity, plasma cytokine levels, and the frequency of circulating Follicular T helper cells (cTfh) and plasmablasts were analyzed by conventional methods.
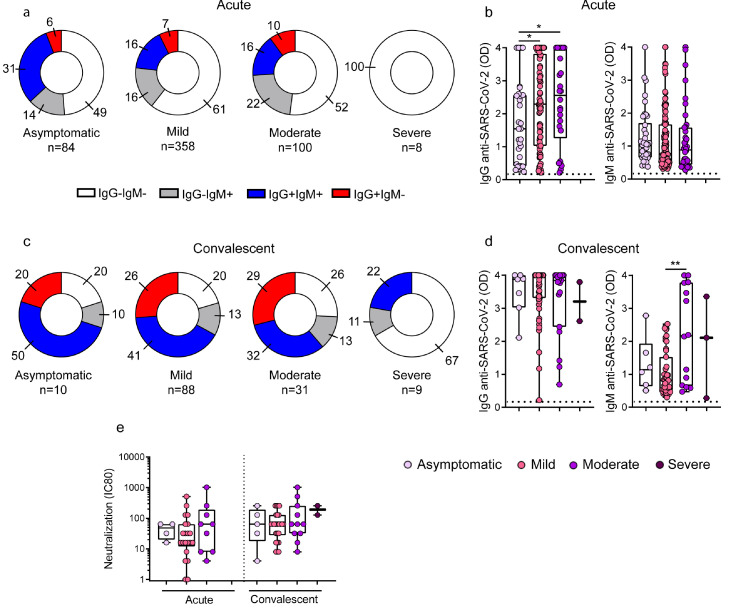
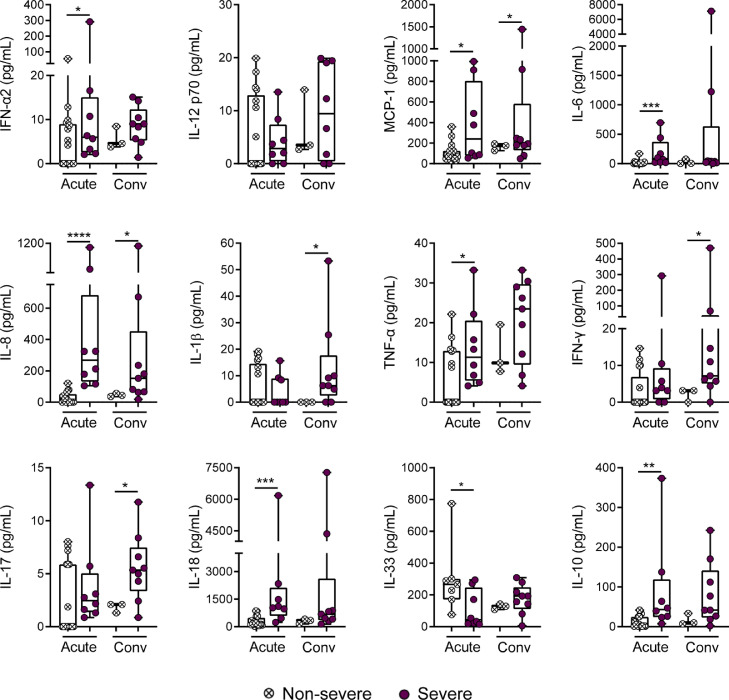
Findings: Fifty-eight percent of the children in the acute phase of infection had no detectable antibodies at the time of sampling while a seronegative status was found in 25% and 12% of convalescent and MIS-C children, respectively. When children in the acute phase of the infection were stratified according disease severity, we found that contrasting with the response of children with asymptomatic, mild and moderate disease, children with severe COVID-19 did not develop any detectable response. A defective antibody response was also observed in the convalescent cohort for children with severe disease at the time of admission. This poor antibody response was associated to both, a low frequency of cTfh and a high plasma concentration of inflammatory cytokines.
Interpretation: A weak and delayed kinetic of antibody response to SARS-CoV-2 together with a systemic pro-inflammatory profile characterize pediatric severe COVID-19. Because comorbidities are highly prevalent in children with severe COVID-19, further studies are needed to clarify their contribution in the weak antibody response observed in severe disease.
Funding: National Agency for Scientific and Technological Promotion from Argentina (IP-COVID-19-0277 and PMO-BID-PICT2018-2548).
Keywords: Disease severity, antibodies, T cells; Pediatric COVID-19.
Copyright © 2021 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest None.
Figures
References
-
- Dong Y., Mo X., Hu Y. Epidemiology of COVID-19 among children in China. Pediatrics. 2020;145(6) - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
