

Diagnosis of cervical plexus tumours by high-frequency ultrasonography
- PMID: 34649505
- PMCID: PMC8515767
- DOI: 10.1186/s12880-021-00682-5
Diagnosis of cervical plexus tumours by high-frequency ultrasonography
Abstract
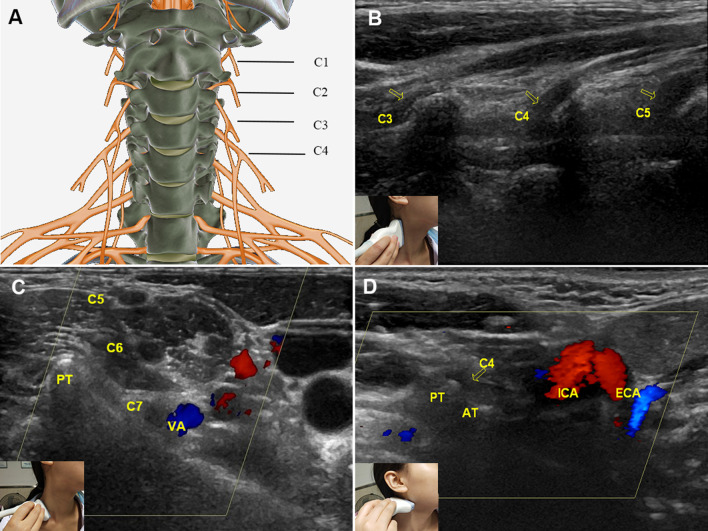
Background: Cervical plexus (CP) tumours are difficult to diagnose because of atypical symptoms. This study aimed to summarize the features of a normal CP and CP tumours observed on high-frequency ultrasonography.
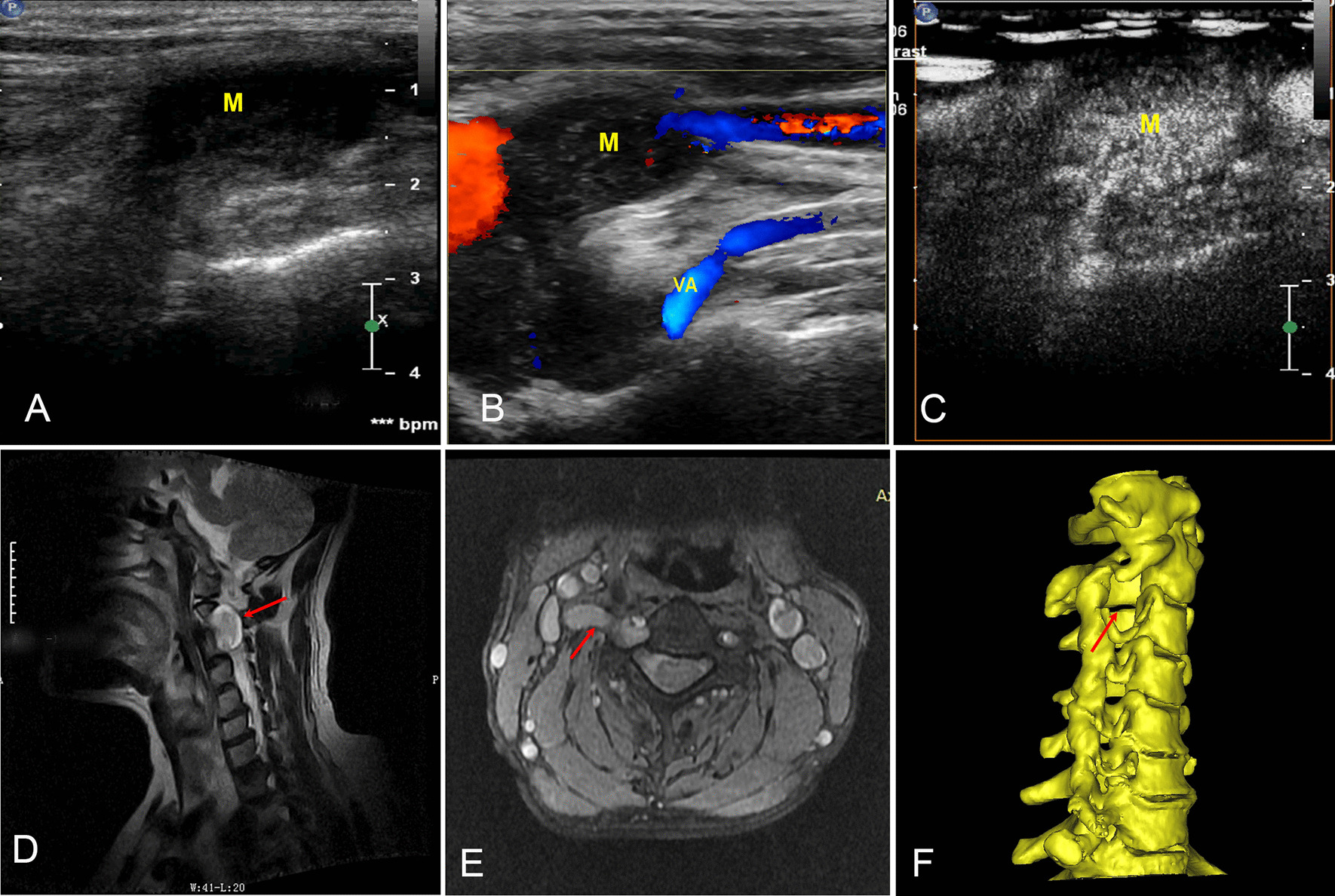
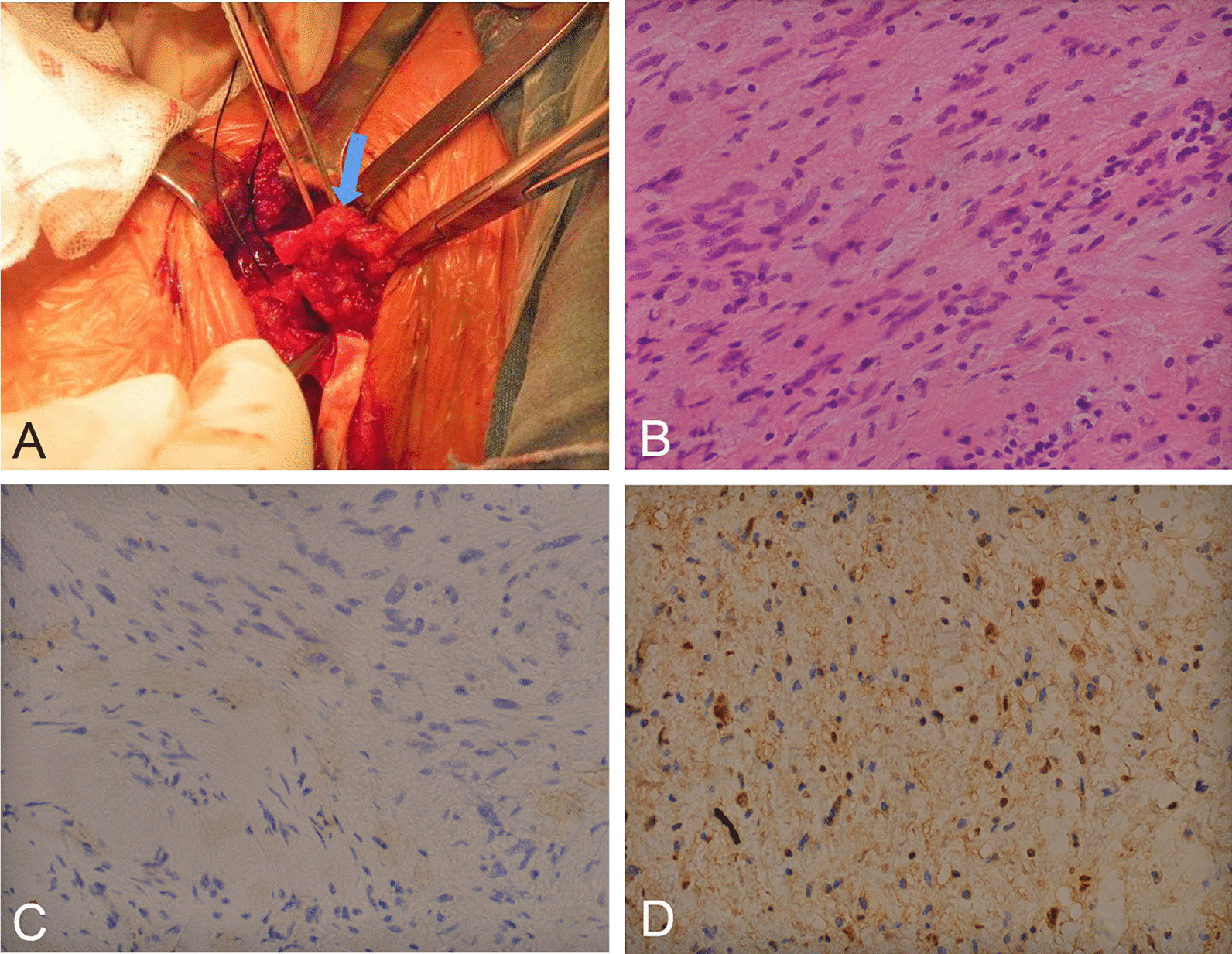
Methods: The ultrasound data of 11 CP tumour patients and 22 normal volunteers were collected. All 11 patients underwent magnetic resonance imaging (MRI), and 4 patients also underwent computed tomography (CT). The imaging data were compared with surgery and pathology data.
Results: The C7 vertebra and bifurcation of the carotid common artery (CCA) were useful anatomic markers for identifying the CP. In contrast to the C1 nerve (22.7%), the C2-4 nerves were well displayed and thinner than the brachial plexus (P < 0.05). CP tumours were more common in females (72.7%) and generally located at C4 (72.7%) on the right side (81.8%). Additionally, the nerve trunk in tumour patients was obviously wider than that in normal controls (7.49 ± 1.03 mm vs 2.67 ± 0.36 mm, P < 0.01). Compared with pathology, the diagnostic rates of CP tumours by MRI, CT and high-frequency ultrasound were 72.7% (8/11), 25% (1/4) and 90.9% (10/11), respectively.
Conclusions: The diagnosis of CP neuropathy is accurate and reliable by high-frequency ultrasound, and the C7 vertebra and bifurcation of the CCA are useful anatomic markers in CP ultrasonography.
Keywords: Cervical plexus; High-frequency ultrasonography; Tumour.
© 2021. The Author(s).
Conflict of interest statement
All authors have no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
