

Evaluation of deep learning-based autosegmentation in breast cancer radiotherapy
- PMID: 34649569
- PMCID: PMC8518257
- DOI: 10.1186/s13014-021-01923-1
Evaluation of deep learning-based autosegmentation in breast cancer radiotherapy
Abstract
Purpose: To study the performance of a proposed deep learning-based autocontouring system in delineating organs at risk (OARs) in breast radiotherapy with a group of experts.
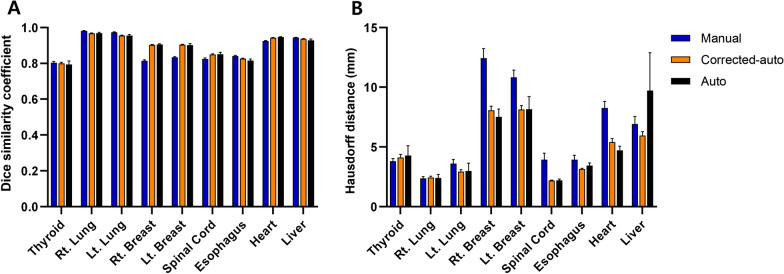
Methods: Eleven experts from two institutions delineated nine OARs in 10 cases of adjuvant radiotherapy after breast-conserving surgery. Autocontours were then provided to the experts for correction. Overall, 110 manual contours, 110 corrected autocontours, and 10 autocontours of each type of OAR were analyzed. The Dice similarity coefficient (DSC) and Hausdorff distance (HD) were used to compare the degree of agreement between the best manual contour (chosen by an independent expert committee) and each autocontour, corrected autocontour, and manual contour. Higher DSCs and lower HDs indicated a better geometric overlap. The amount of time reduction using the autocontouring system was examined. User satisfaction was evaluated using a survey.
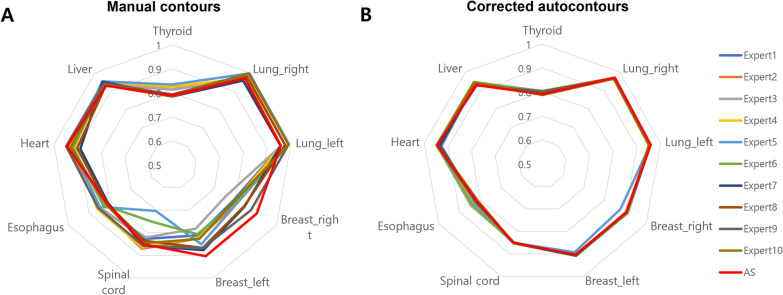
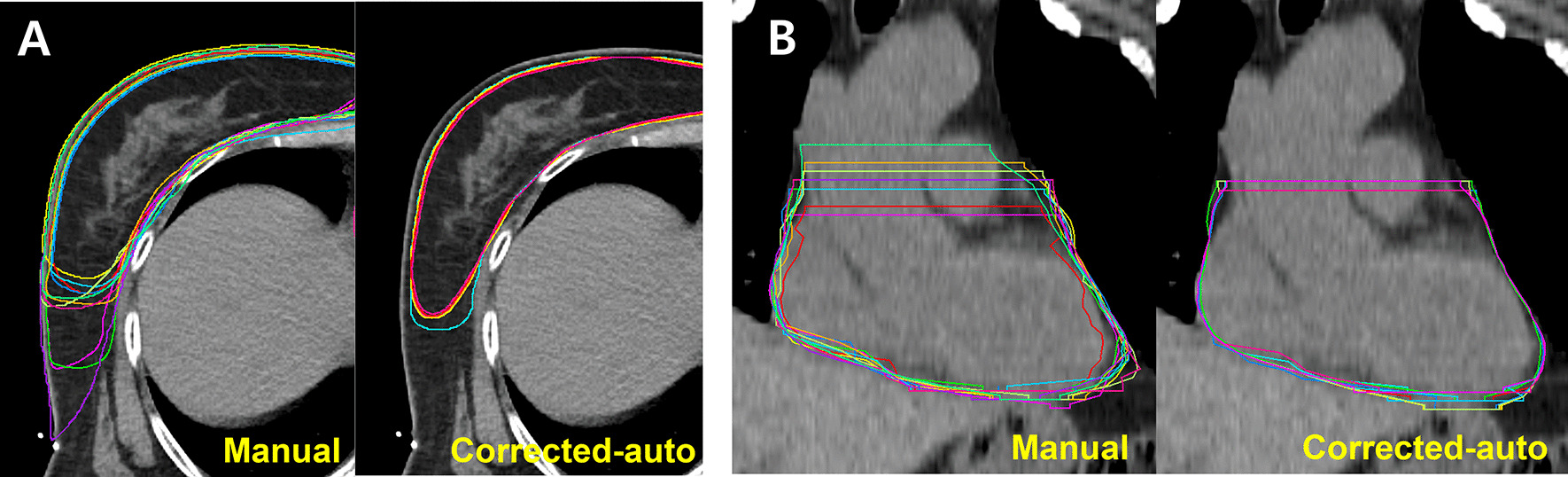
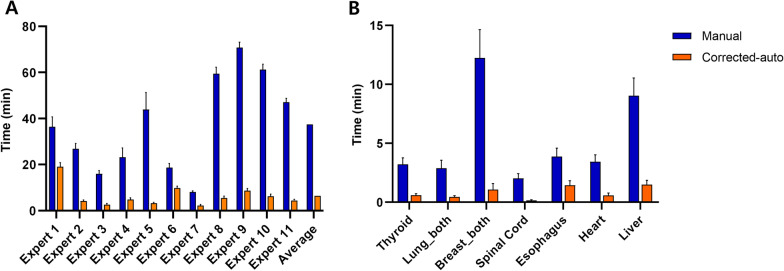
Results: Manual contours, corrected autocontours, and autocontours had a similar accuracy in the average DSC value (0.88 vs. 0.90 vs. 0.90). The accuracy of autocontours ranked the second place, based on DSCs, and the first place, based on HDs among the manual contours. Interphysician variations among the experts were reduced in corrected autocontours, compared to variations in manual contours (DSC: 0.89-0.90 vs. 0.87-0.90; HD: 4.3-5.8 mm vs. 5.3-7.6 mm). Among the manual delineations, the breast contours had the largest variations, which improved most significantly with the autocontouring system. The total mean times for nine OARs were 37 min for manual contours and 6 min for corrected autocontours. The results of the survey revealed good user satisfaction.
Conclusions: The autocontouring system had a similar performance in OARs as that of the experts' manual contouring. This system can be valuable in improving the quality of breast radiotherapy and reducing interphysician variability in clinical practice.
Keywords: Autocontouring; Breast; Organs at risk; Radiotherapy.
© 2021. The Author(s).
Conflict of interest statement
None
Figures
References
-
- Jiang F, Grigorev A, Rho S, Tian Z, Fu Y, Jifara W, et al. Medical image semantic segmentation based on deep learning. Neural Comput Appl. 2018;29(5):1257–1265. doi: 10.1007/s00521-017-3158-6. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
