

Bronchus-blocked ultrasound-guided percutaneous transthoracic needle biopsy (BUS-PTNB) for intubated patients with severe lung diseases
- PMID: 34649600
- PMCID: PMC8515780
- DOI: 10.1186/s13054-021-03782-4
Bronchus-blocked ultrasound-guided percutaneous transthoracic needle biopsy (BUS-PTNB) for intubated patients with severe lung diseases
Abstract
Background: Examinations based on lung tissue specimen can play a significant role in the diagnosis for critically ill and intubated patients with lung infiltration. However, severe complications including tension pneumothorax and intrabronchial hemorrhage limit the application of needle biopsy.
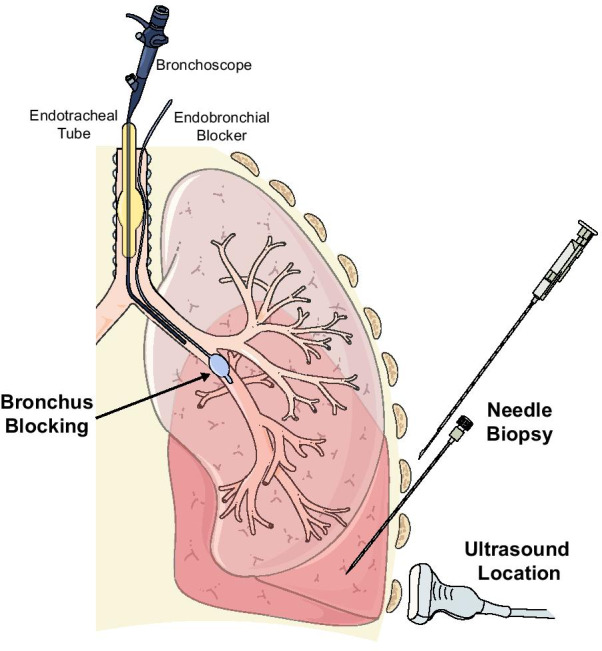
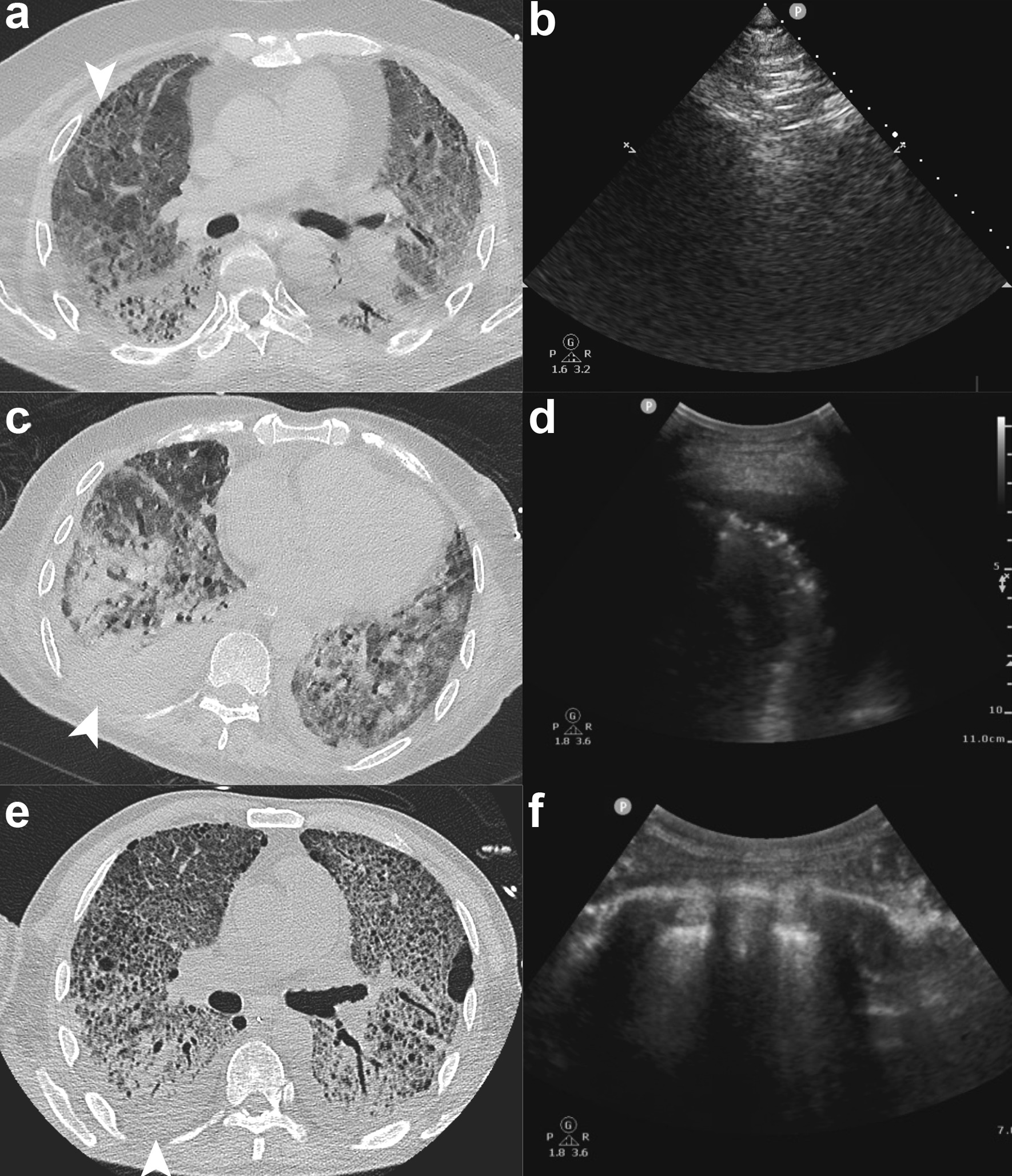
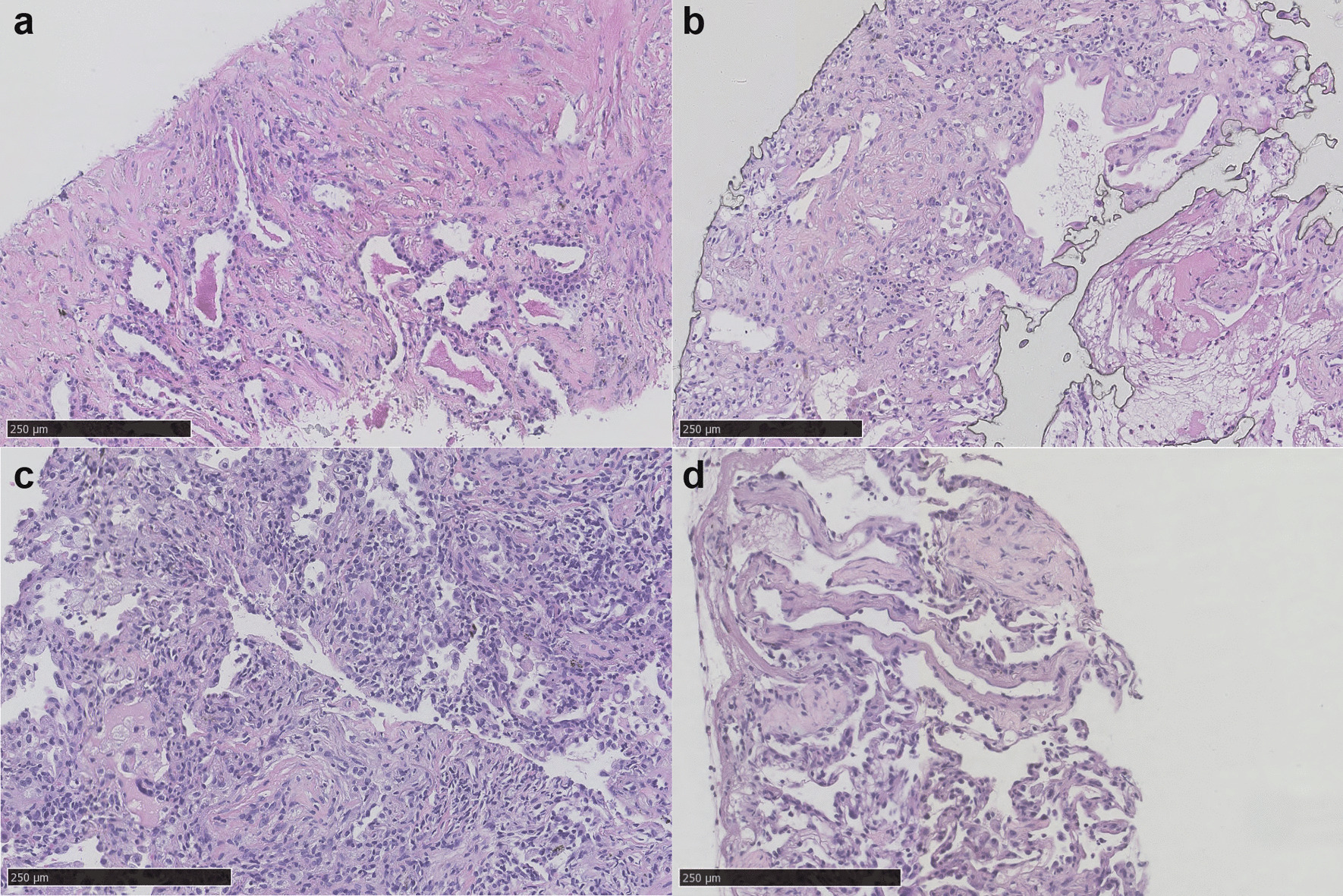
Methods: A refined needle biopsy technique, named bronchus-blocked ultrasound-guided percutaneous transthoracic needle biopsy (BUS-PTNB), was performed on four intubated patients between August 2020 and April 2021. BUS-PTNB was done at bedside, following an EPUBNOW (evaluation, preparation, ultrasound location, bronchus blocking, needle biopsy, observation, and withdrawal of blocker) workflow. Parameters including procedure feasibility, sample acquisition, perioperative conditions, and complications were observed. Tissue specimens were sent to pathological examinations and microbial tests.
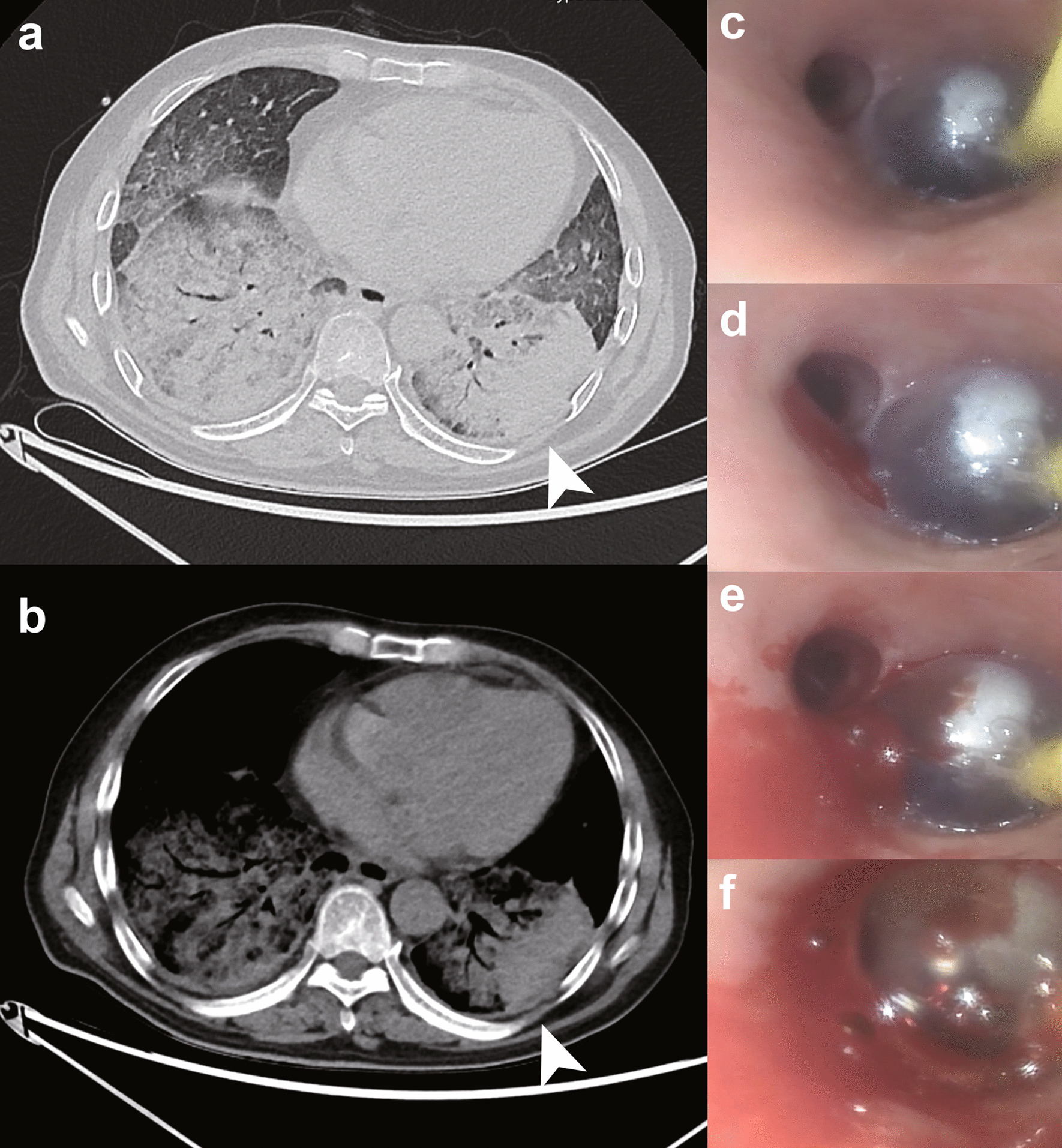
Results: Adequate specimens were successfully obtained from four patients. Diagnosis and treatment were correspondingly refined based on pathological and microbial tests. Intrabronchial hemorrhage occurred in patient 1 but was stopped by endobronchial blocker. Mild pneumothorax happened in patient 4 due to little air leakage, and closed thoracic drainage was placed. During the procedure, peripheral capillary hemoglobin oxygen saturation (SPO2), blood pressure, and heart rate of patient 4 fluctuated but recovered quickly. Vital signs were stable for patient 1-3.
Conclusions: BUS-PTNB provides a promising, practical and feasible method in acquiring tissue specimen for critically ill patients under intratracheal intubation. It may facilitate the pathological diagnosis or other tissue-based tests for intubated patients and improve clinical outcomes.
Keywords: Bronchoscopy; Endobronchial blocker; Intubation; Needle biopsy; Sonography.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Clinical role, safety and diagnostic accuracy of percutaneous transthoracic needle biopsy in the evaluation of pulmonary consolidation.Respir Res. 2019 Jan 31;20(1):23. doi: 10.1186/s12931-019-0982-5. Respir Res. 2019. PMID: 30704502 Free PMC article.
-
Open Bronchus Sign on CT: A Risk Factor for Hemoptysis after Percutaneous Transthoracic Biopsy.Korean J Radiol. 2018 Sep-Oct;19(5):880-887. doi: 10.3348/kjr.2018.19.5.880. Epub 2018 Aug 6. Korean J Radiol. 2018. PMID: 30174477 Free PMC article.
-
The clinical performance of robotic assisted navigation system versus conventional freehand technique for percutaneous transthoracic needle biopsy.Sci Rep. 2025 Feb 18;15(1):5980. doi: 10.1038/s41598-025-87987-5. Sci Rep. 2025. PMID: 39966451 Free PMC article.
-
Clinical updates of approaches for biopsy of pulmonary lesions based on systematic review.BMC Pulm Med. 2018 Sep 3;18(1):146. doi: 10.1186/s12890-018-0713-6. BMC Pulm Med. 2018. PMID: 30176840 Free PMC article.
-
2020 Clinical Practice Guideline for Percutaneous Transthoracic Needle Biopsy of Pulmonary Lesions: A Consensus Statement and Recommendations of the Korean Society of Thoracic Radiology.Korean J Radiol. 2021 Feb;22(2):263-280. doi: 10.3348/kjr.2020.0137. Epub 2020 Nov 19. Korean J Radiol. 2021. PMID: 33236542 Free PMC article. Review.
References
-
- Kyo M, Hosokawa K, Ohshimo S, Kida Y, Tanabe Y, Shime N. Prognosis of pathogen-proven acute respiratory distress syndrome diagnosed from a protocol that includes bronchoalveolar lavage: a retrospective observational study. J Intensive Care. 2020;8(1):1–7. doi: 10.1186/s40560-020-00469-w. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
