

Effectiveness of therapeutic heparin versus prophylactic heparin on death, mechanical ventilation, or intensive care unit admission in moderately ill patients with covid-19 admitted to hospital: RAPID randomised clinical trial
- PMID: 34649864
- PMCID: PMC8515466
- DOI: 10.1136/bmj.n2400
Effectiveness of therapeutic heparin versus prophylactic heparin on death, mechanical ventilation, or intensive care unit admission in moderately ill patients with covid-19 admitted to hospital: RAPID randomised clinical trial
Abstract
Objective: To evaluate the effects of therapeutic heparin compared with prophylactic heparin among moderately ill patients with covid-19 admitted to hospital wards.
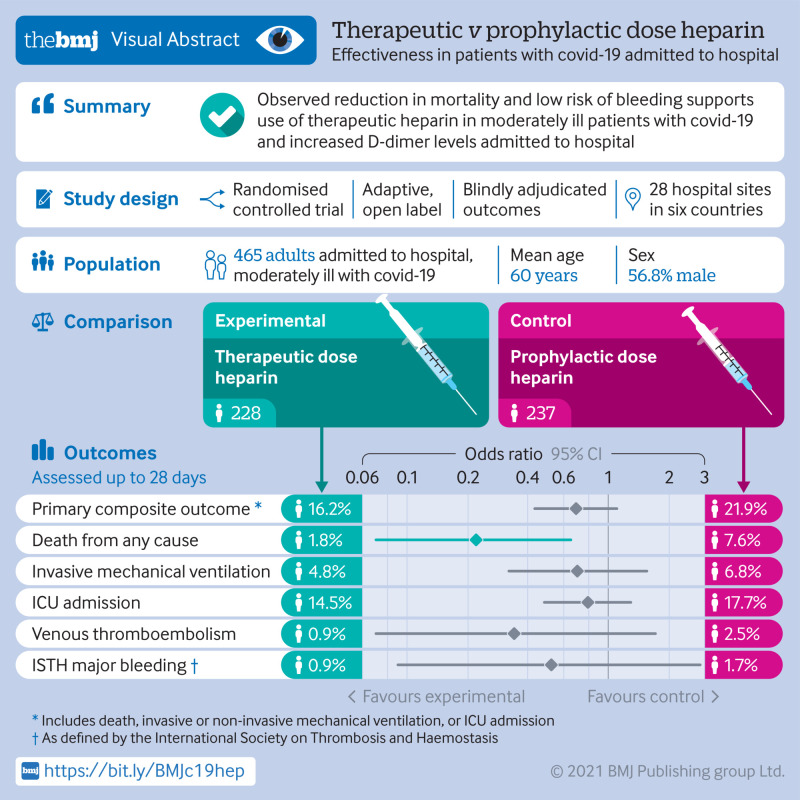
Design: Randomised controlled, adaptive, open label clinical trial.
Setting: 28 hospitals in Brazil, Canada, Ireland, Saudi Arabia, United Arab Emirates, and US.
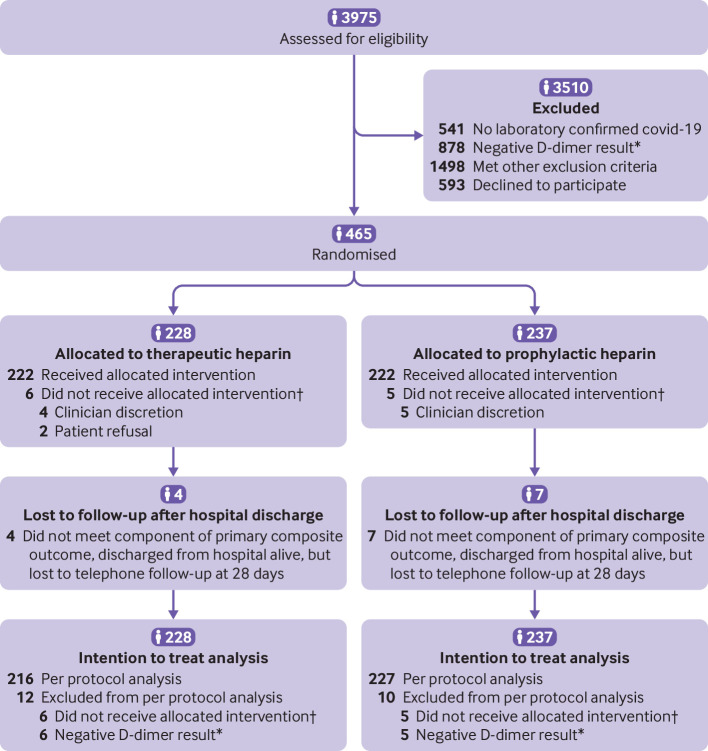
Participants: 465 adults admitted to hospital wards with covid-19 and increased D-dimer levels were recruited between 29 May 2020 and 12 April 2021 and were randomly assigned to therapeutic dose heparin (n=228) or prophylactic dose heparin (n=237).
Interventions: Therapeutic dose or prophylactic dose heparin (low molecular weight or unfractionated heparin), to be continued until hospital discharge, day 28, or death.
Main outcome measures: The primary outcome was a composite of death, invasive mechanical ventilation, non-invasive mechanical ventilation, or admission to an intensive care unit, assessed up to 28 days. The secondary outcomes included all cause death, the composite of all cause death or any mechanical ventilation, and venous thromboembolism. Safety outcomes included major bleeding. Outcomes were blindly adjudicated.
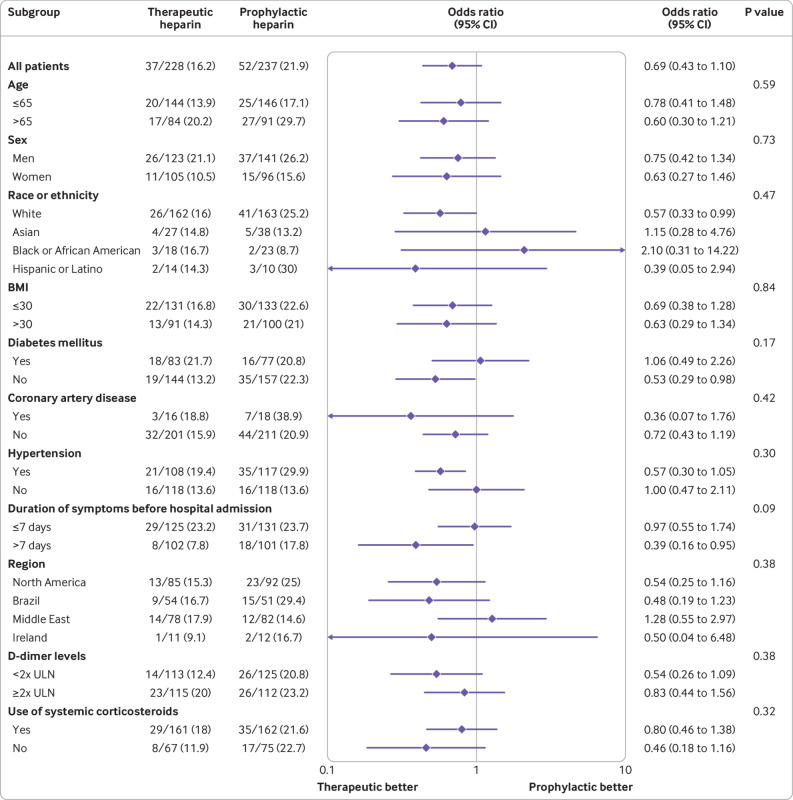
Results: The mean age of participants was 60 years; 264 (56.8%) were men and the mean body mass index was 30.3 kg/m2. At 28 days, the primary composite outcome had occurred in 37/228 patients (16.2%) assigned to therapeutic heparin and 52/237 (21.9%) assigned to prophylactic heparin (odds ratio 0.69, 95% confidence interval 0.43 to 1.10; P=0.12). Deaths occurred in four patients (1.8%) assigned to therapeutic heparin and 18 patients (7.6%) assigned to prophylactic heparin (0.22, 0.07 to 0.65; P=0.006). The composite of all cause death or any mechanical ventilation occurred in 23 patients (10.1%) assigned to therapeutic heparin and 38 (16.0%) assigned to prophylactic heparin (0.59, 0.34 to 1.02; P=0.06). Venous thromboembolism occurred in two patients (0.9%) assigned to therapeutic heparin and six (2.5%) assigned to prophylactic heparin (0.34, 0.07 to 1.71; P=0.19). Major bleeding occurred in two patients (0.9%) assigned to therapeutic heparin and four (1.7%) assigned to prophylactic heparin (0.52, 0.09 to 2.85; P=0.69).
Conclusions: In moderately ill patients with covid-19 and increased D-dimer levels admitted to hospital wards, therapeutic heparin was not significantly associated with a reduction in the primary outcome but the odds of death at 28 days was decreased. The risk of major bleeding appeared low in this trial.
Trial registration: ClinicalTrials.gov NCT04362085.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: MS reports receiving funding from Task 54, Defense Research Development Canada, Department of National Defense, Ottawa, Canada (to institution), St Michael’s Hospital Foundation, Toronto, Canada (to institution), St Joseph’s Health Centre Foundation, Toronto, Canada (to institution), International Network of Venous Thromboembolism Clinical Research Networks (INVENT) Kickstarter Award (to institution) during the conduct of this study. LBK reports receiving funding from the INVENT Kickstarter Award during the conduct of the study. FNA reports receiving Science Foundation Ireland, Enterprise Ireland, IDA Ireland COVID-19 Rapid Response Funding Call 20/COV/0157 (to Institution; University College Dublin) during the conduct of this study; and grants or contracts from Sanofi, Daiichi-Sankyo, Irish Health Research Board (a state agency under the Department of Health, supporting and funding health and social care research), and Bayer; and reports patent submitted (European Application No 20166826.6) outside of the submitted work. LAC reports receiving honorariums for lectures and presentations for Bristol Meyers Squibb, Pfizer, Bayer, Boehringer Ingelheim, Leo Pharma, Sanofi, The Academy for Continued Advancement in Healthcare Education outside of the submitted work. PDJ reports receiving research grant funding from Bayer, Takeda, CSL Behring outside of the submitted work and reports receiving funding from SEAMO (South-eastern Ontario Academic Medical Organization) COIVD-19 Innovation Fund during the conduct of this study. DL reports receiving research support from Bayer, Biomarin, CSL-Behring, Octapharma, Sanofi; and serving on Data Safety Monitoring and Advisory Boards for Biomarin, CSL Behring, Takeda, Sanofi, and Spark outside of the submitted work. MCa reports grant or contracts from Bristol Meyers Squibb, Leo Pharma, Pfizer (to institution); consulting fees from Bayer, Pfizer, Bristol Meyers Squibb, Sanofi, Servier, Leo Pharma (to institution) outside of the submitted work. CC reports stock options from BioCogniv, Burlington, Vermont, USA outside of the submitted work. CW reports receiving payment or honorariums for speaking engagements from Leo Pharma, Pfizer, Bristol Meyers Squibb-Pfizer, and Servier and serving on advisory board meetings for LEO Pharma, Pfizer, Bristol Meyers Squibb-Pfizer, Servier outside of the submitted work. KD reports receiving honorariums from LEO Pharma and Pfizer outside of the submitted work. ERA reports receiving funding from 2020 TD Community Health Solutions Fund COVID-19 research grant (to institution) during the conduct of this study; honorariums from Pfizer and Bayer; support for attending meetings and/or travel from Pfizer, and participation in advisory board for Tavalisse outside of the submitted work. MF reports consulting fees from Pine Trees Health outside of the submitted work. SM reports grants and personal fees from Daiichy Sankyo, grants and personal fees from Bayer, Pfizer, and Boehringer-Ingelheim, personal fees from Portola, Abbvie, Bristol Meyers Squibb-Pfizer, and Sanofi, outside the submitted work. AYYL reports receiving consulting fees from LEO Pharma; payment or honorariums for speaking engagements and/or consulting from LEO Pharma and Pfizer, and serving on a data safety monitoring board or advisory board for CONNECTS program (COVID-19 clinical trials involving anticoagulation) outside of the submitted work. MC reports receiving an honorarium from the International Society on Thrombosis and Haemostasis outside of the submitted work. PJü reports receiving funding from Task 54, Defense Research Development Canada, Department of National Defense, Ottawa, Canada (to institution), St Michael’s Hospital Foundation, Toronto, Canada (to institution), St Joseph’s Health Centre Foundation, Toronto, Canada (to institution), International Network of Venous Thromboembolism Clinical Research Networks (INVENT) Kickstarter Award (to institution) during the conduct of this study; receiving a grant from Appili Therapeutics (to the institution); payment for participation in advisory boards and/or consulting for Amgen and Fresenius (to the institution); honorariums and travel reimbursement from Amgen, Ava, and Fresenius (to the institution); participation in advisory boards and/or consulting for Amgen and Fresenius; and serves as unpaid member of the steering group of trials funded by Appili Therapeutics, Terumo, and Abbott Vascular outside of the submitted work.
Figures
Update of
-
Heparin for Moderately Ill Patients with Covid-19.medRxiv [Preprint]. 2021 Jul 12:2021.07.08.21259351. doi: 10.1101/2021.07.08.21259351. medRxiv. 2021. Update in: BMJ. 2021 Oct 14;375:n2400. doi: 10.1136/bmj.n2400. PMID: 34268513 Free PMC article. Updated. Preprint.
Comment in
-
In patients hospitalized with COVID-19, therapeutic- vs. prophylactic-dose heparin did not reduce a composite outcome at 28 d.Ann Intern Med. 2022 Feb;175(2):JC16. doi: 10.7326/J21-0020. Epub 2022 Feb 1. Ann Intern Med. 2022. PMID: 35099997
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous