

TUBB3 Arg262His causes a recognizable syndrome including CFEOM3, facial palsy, joint contractures, and early-onset peripheral neuropathy
- PMID: 34652576
- PMCID: PMC8656246
- DOI: 10.1007/s00439-021-02379-9
TUBB3 Arg262His causes a recognizable syndrome including CFEOM3, facial palsy, joint contractures, and early-onset peripheral neuropathy
Abstract
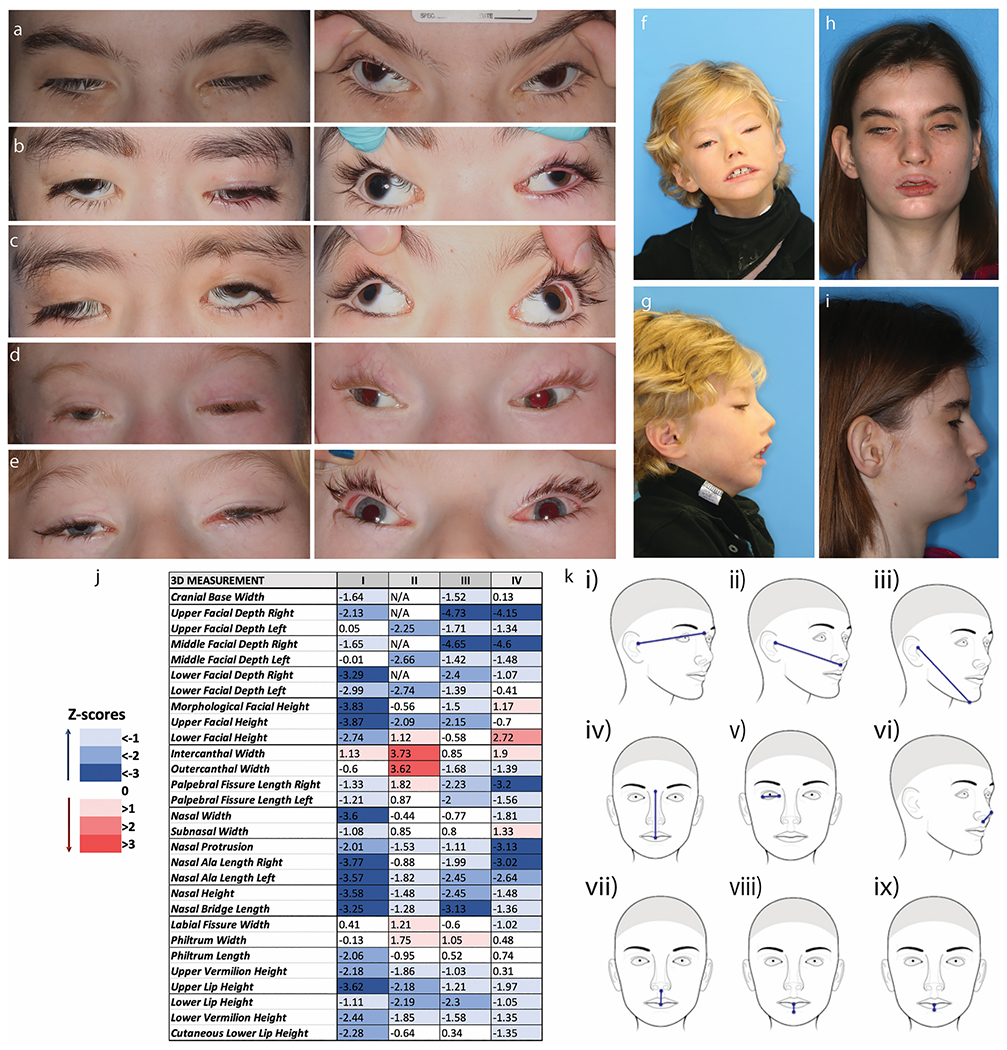
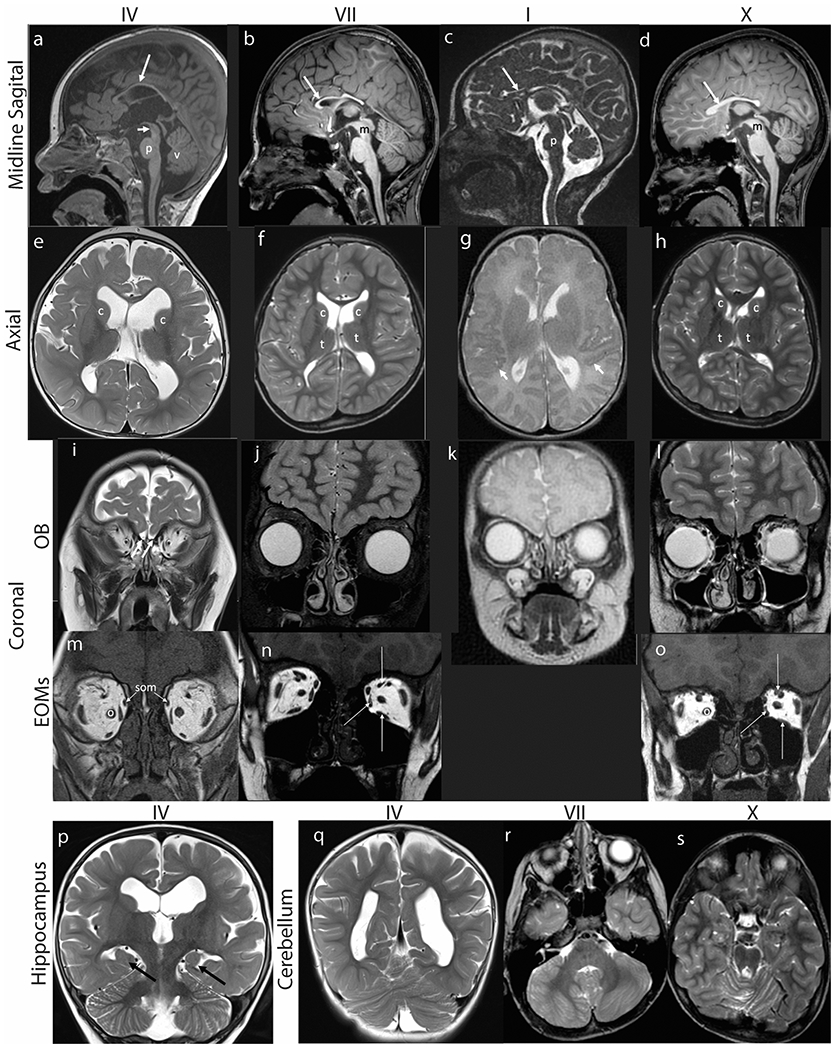
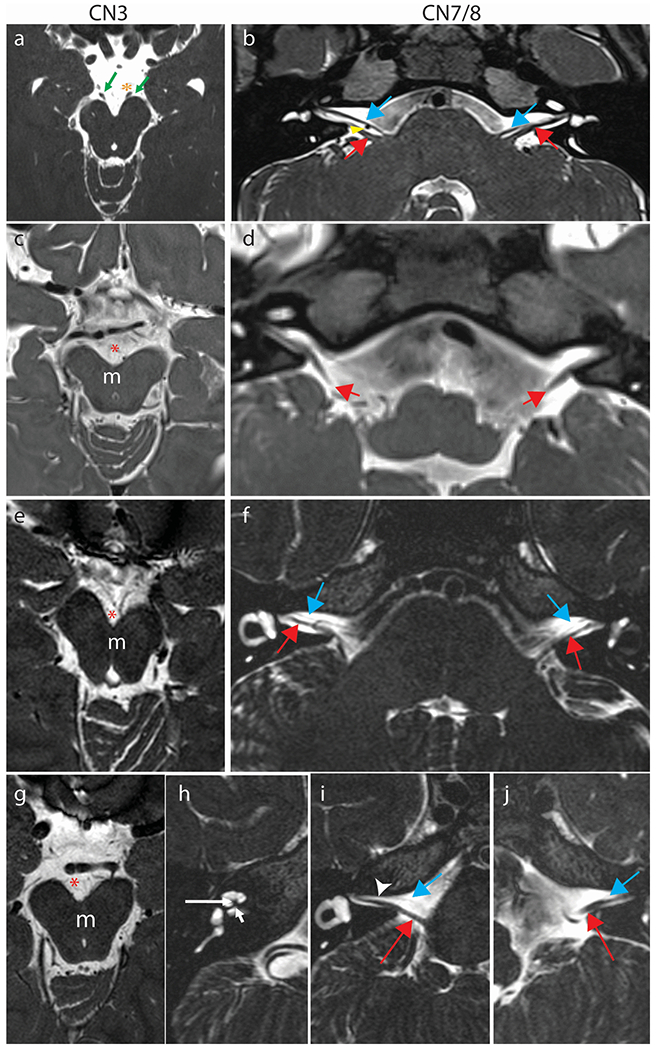
Microtubules are formed from heterodimers of alpha- and beta-tubulin, each of which has multiple isoforms encoded by separate genes. Pathogenic missense variants in multiple different tubulin isoforms cause brain malformations. Missense mutations in TUBB3, which encodes the neuron-specific beta-tubulin isotype, can cause congenital fibrosis of the extraocular muscles type 3 (CFEOM3) and/or malformations of cortical development, with distinct genotype-phenotype correlations. Here, we report fourteen individuals from thirteen unrelated families, each of whom harbors the identical NM_006086.4 (TUBB3):c.785G>A (p.Arg262His) variant resulting in a phenotype we refer to as the TUBB3 R262H syndrome. The affected individuals present at birth with ptosis, ophthalmoplegia, exotropia, facial weakness, facial dysmorphisms, and, in most cases, distal congenital joint contractures, and subsequently develop intellectual disabilities, gait disorders with proximal joint contractures, Kallmann syndrome (hypogonadotropic hypogonadism and anosmia), and a progressive peripheral neuropathy during the first decade of life. Subsets may also have vocal cord paralysis, auditory dysfunction, cyclic vomiting, and/or tachycardia at rest. All fourteen subjects share a recognizable set of brain malformations, including hypoplasia of the corpus callosum and anterior commissure, basal ganglia malformations, absent olfactory bulbs and sulci, and subtle cerebellar malformations. While similar, individuals with the TUBB3 R262H syndrome can be distinguished from individuals with the TUBB3 E410K syndrome by the presence of congenital and acquired joint contractures, an earlier onset peripheral neuropathy, impaired gait, and basal ganglia malformations.
© 2021. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
Figures

References
-
- Bahi-Buisson N, Poirier K, Fourniol F, Saillour Y, Valence S, Lebrun N, Hully M, Bianco CF, Boddaert N, Elie C, Lascelles K, Souville I, Consortium LI-T, Beldjord C, Chelly J (2014) The wide spectrum of tubulinopathies: what are the key features for the diagnosis? Brain 137: 1676–700. doi: 10.1093/brain/awu082 - DOI - PubMed
-
- Bonomi M, Vezzoli V, Krausz C, Guizzardi F, Vezzani S, Simoni M, Bassi I, Duminuco P, Di lorgi N, Giavoli C, Pizzocaro A, Russo G, Moro M, Fatti L, Ferlin A, Mazzanti L, Zatelli MC, Cannavo S, Isidori AM, Pincelli AI, Prodam F, Mancini A, Limone P, Tanda ML, Gaudino R, Salerno M, Francesca P, Maghnie M, Maggi M, Persani L, Italian Network on Central H, Italian Network on Central H (2018) Characteristics of a nationwide cohort of patients presenting with isolated hypogonadotropic hypogonadism (IHH). Eur J Endocrinol 178: 23–32. doi: 10.1530/EJE-17-0065 - DOI - PubMed
-
- Brinkley JF, Fisher S, Harris MP, Holmes G, Hooper JE, Jabs EW, Jones KL, Kesselman C, Klein OD, Maas RL, Marazita ML, Selleri L, Spritz RA, van Bakel H, Visel A, Williams TJ, Wysocka J, FaceBase C, Chai Y (2016) The FaceBase Consortium: a comprehensive resource for craniofacial researchers. Development 143: 2677–88. doi: 10.1242/dev.135434 - DOI - PMC - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
- Z99 HG999999/ImNIH/Intramural NIH HHS/United States
- ZIA HD008919/NH/NIH HHS/United States
- K12 EY016335/EY/NEI NIH HHS/United States
- ZIA HG200389/ImNIH/Intramural NIH HHS/United States
- K08 EY027850/EY/NEI NIH HHS/United States
- ZIA HD008919/ImNIH/Intramural NIH HHS/United States
- 5K12EY016335/EY/NEI NIH HHS/United States
- U01HD079068/NH/NIH HHS/United States
- ZIA DE000746/ImNIH/Intramural NIH HHS/United States
- P50 HD105351/HD/NICHD NIH HHS/United States
- 5K08EY027850/EY/NEI NIH HHS/United States
- U01 HD079068/HD/NICHD NIH HHS/United States
- ZIA HG200389-08/NH/NIH HHS/United States
- NIDCD Intramural Research Program/DC/NIDCD NIH HHS/United States
- NIH Director's Common Fund to the NIH Undiagnosed Diseases Program/NH/NIH HHS/United States
- ZIA DE000746-06/NH/NIH HHS/United States
- U54 HD090255/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
