

Phase III Trial Adding Vincristine-Topotecan-Cyclophosphamide to the Initial Treatment of Patients With Nonmetastatic Ewing Sarcoma: A Children's Oncology Group Report
- PMID: 34652968
- PMCID: PMC8677904
- DOI: 10.1200/JCO.21.00358
Phase III Trial Adding Vincristine-Topotecan-Cyclophosphamide to the Initial Treatment of Patients With Nonmetastatic Ewing Sarcoma: A Children's Oncology Group Report
Erratum in
-
Erratum.J Clin Oncol. 2022 Jul 20;40(21):2393. doi: 10.1200/JCO.22.01234. J Clin Oncol. 2022. PMID: 35839523 Free PMC article. No abstract available.
Abstract
Purpose: The primary aim of this phase III randomized trial was to test whether the addition of vincristine, topotecan, and cyclophosphamide (VTC) to interval compressed chemotherapy improved survival outcomes for patients with previously untreated nonmetastatic Ewing sarcoma.
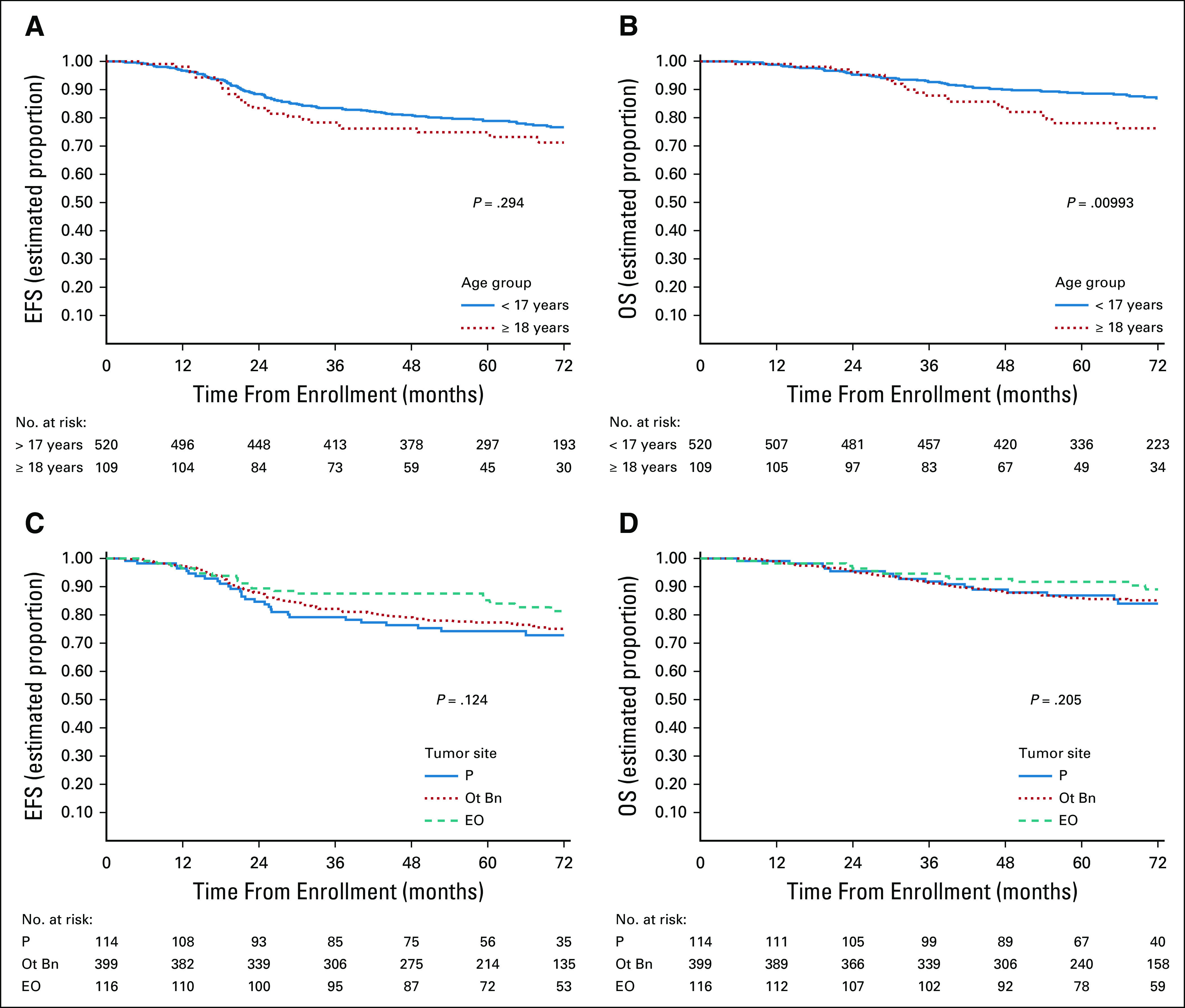
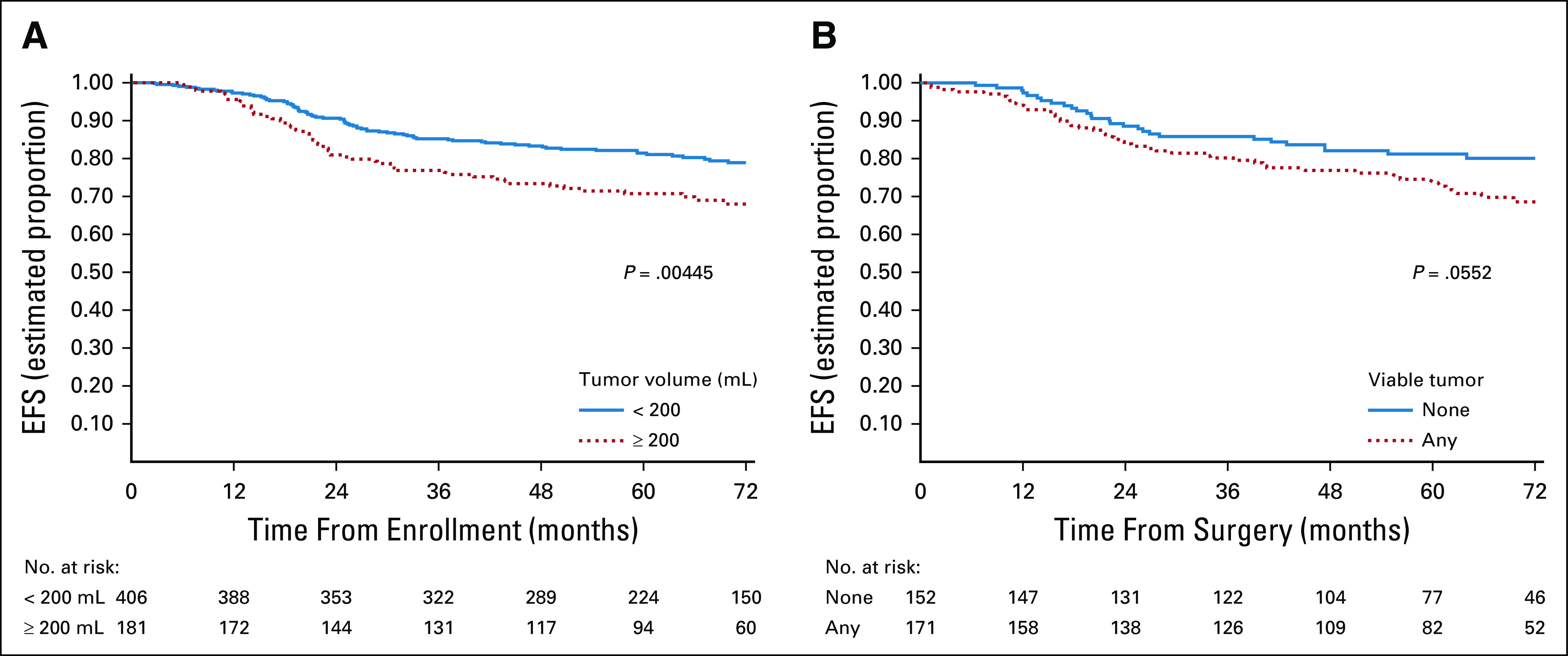
Methods: Patients were randomly assigned to receive standard five-drug interval compressed chemotherapy (regimen A) for 17 cycles or experimental therapy with five cycles of VTC within the 17 cycles (regimen B). Patients were stratified by age at diagnosis (< 18 years and ≥18 years) and tumor site (pelvic bone, nonpelvic bone, and extraosseous). Tumor volume at diagnosis was categorized as < 200 mL or ≥ 200 mL. Local control occurred following six cycles. Histologic response was categorized as no viable or any viable tumor. Event-free survival (EFS) and overall survival (OS) were compared between randomized groups with stratified log-rank tests.
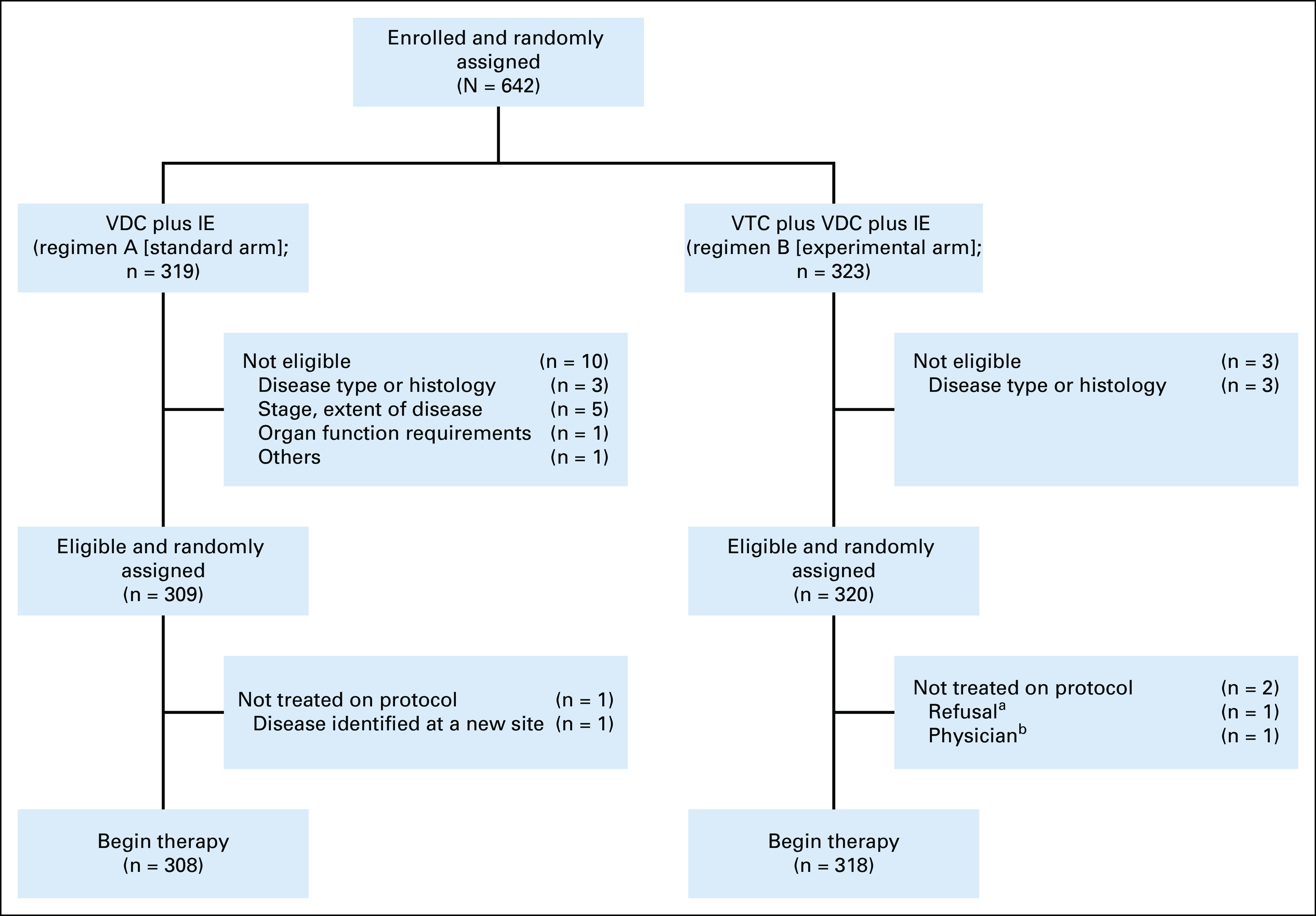
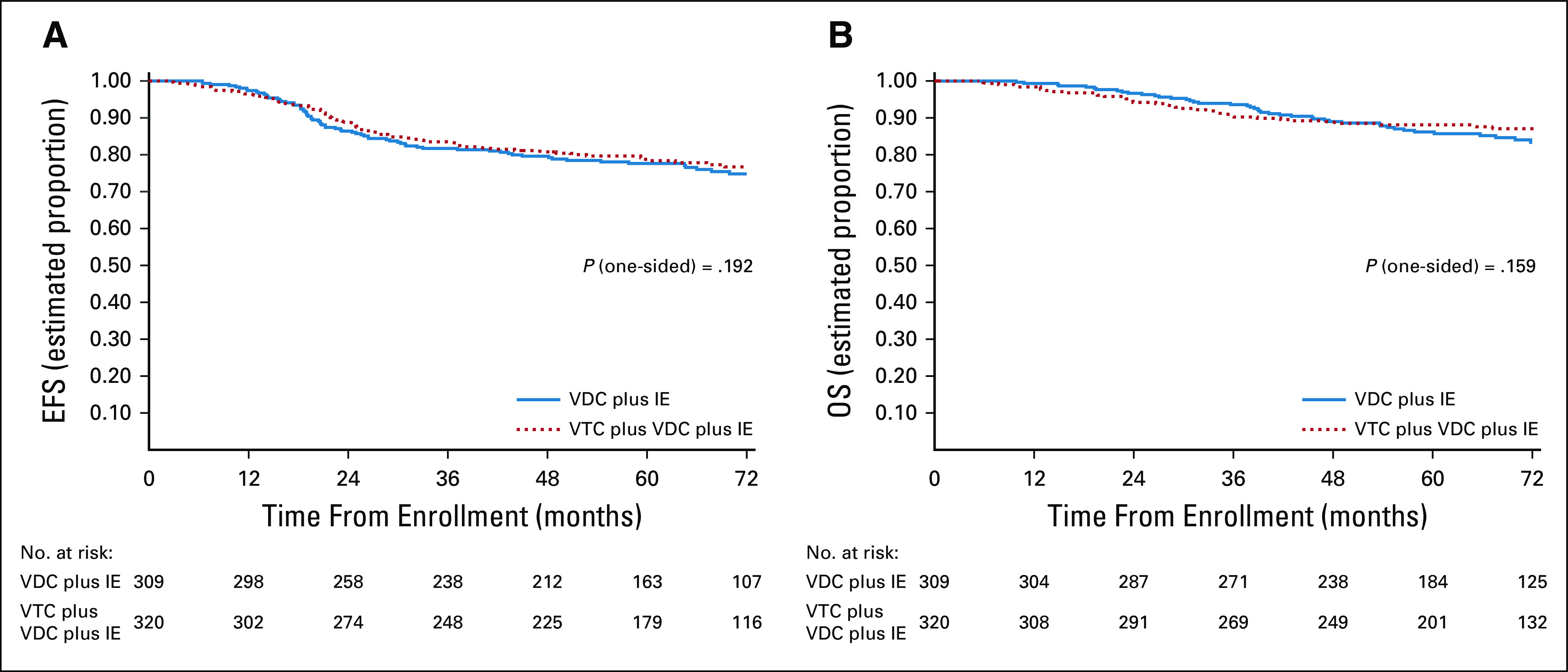
Results: Of 642 enrolled patients, 309 eligible patients received standard and 320 received experimental therapy. The 5-year EFS and OS were 78% and 87%, respectively. There was no difference in survival outcomes between randomized groups (5-year EFS regimen A v regimen B, 78% v 79%; P = .192; 5-year OS 86% v 88%; P = .159). Age and primary site did not affect the risk of an EFS event. However, age ≥ 18 years was associated with an increased risk of death at 5 years (hazard ratio 1.84; 95% CI, 1.15 to 2.96; P = .009). The 5-year EFS rates for patients with pelvic, nonpelvic bone, and extraosseous primary tumors were 75%, 78%, and 85%, respectively. Tumor volume ≥ 200 mL was significantly associated with lower EFS.
Conclusion: While VTC added to five-drug interval compressed chemotherapy did not improve survival, these outcomes represent the best survival estimates to date for patients with previously untreated nonmetastatic Ewing sarcoma.
Trial registration: ClinicalTrials.gov NCT01231906.
Conflict of interest statement
Figures
Comment in
-
Regarding the Children's Oncology Group AEWS1031 Trial for Ewing Sarcoma.J Clin Oncol. 2022 May 1;40(13):1506. doi: 10.1200/JCO.21.02546. Epub 2022 Mar 2. J Clin Oncol. 2022. PMID: 35235371 No abstract available.
-
Reply to J.-G. Wang et al.J Clin Oncol. 2022 May 1;40(13):1507-1508. doi: 10.1200/JCO.21.02922. Epub 2022 Mar 2. J Clin Oncol. 2022. PMID: 35235382 Free PMC article. No abstract available.
References
-
- Grier HE, Krailo MD, Tarbell NJ, et al. : Addition of ifosfamide and etoposide to standard chemotherapy for Ewing's sarcoma and primitive neuroectodermal tumor of bone. N Engl J Med 348:694-701, 2003 - PubMed
-
- Saylors RL III, Stine KC, Sullivan J, et al. : Cyclophosphamide plus topotecan in children with recurrent or refractory solid tumors: A Pediatric Oncology Group phase II study. J Clin Oncol 19:3463-3469, 2001 - PubMed
-
- Hunold A, Weddeling N, Paulussen M, et al. : Topotecan and cyclophosphamide in patients with refractory or relapsed Ewing tumors. Pediatr Blood Cancer 47:795-800, 2006 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
